

Decreased Appendicular Skeletal Muscle Mass is Associated with Poor Outcomes after ST-Segment Elevation Myocardial Infarction
- PMID: 32132340
- PMCID: PMC7840163
- DOI: 10.5551/jat.52282
Decreased Appendicular Skeletal Muscle Mass is Associated with Poor Outcomes after ST-Segment Elevation Myocardial Infarction
Abstract
Aim: The importance of sarcopenia in cardiovascular diseases has been recently demonstrated. This study aims to examine whether skeletal muscle mass (SMM), an important component of sarcopenia, is associated with an increased risk of poor outcome in patients after ST-segment elevation myocardial infarction (STEMI).
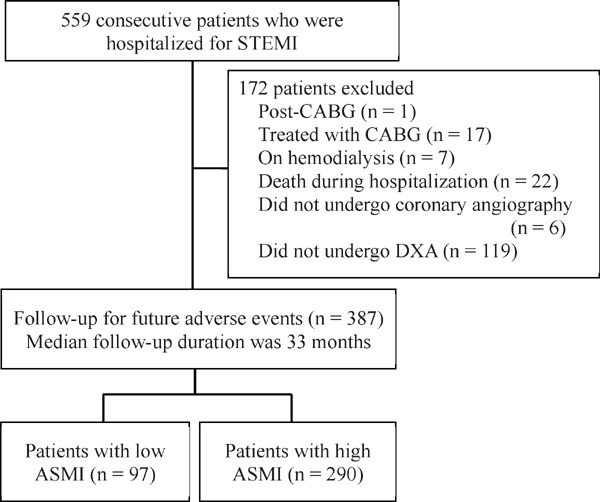
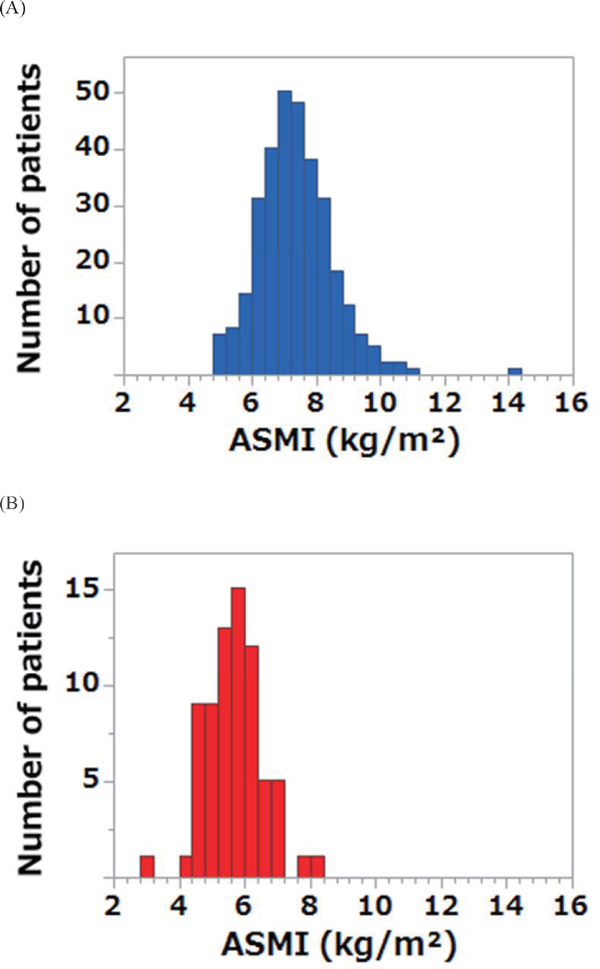
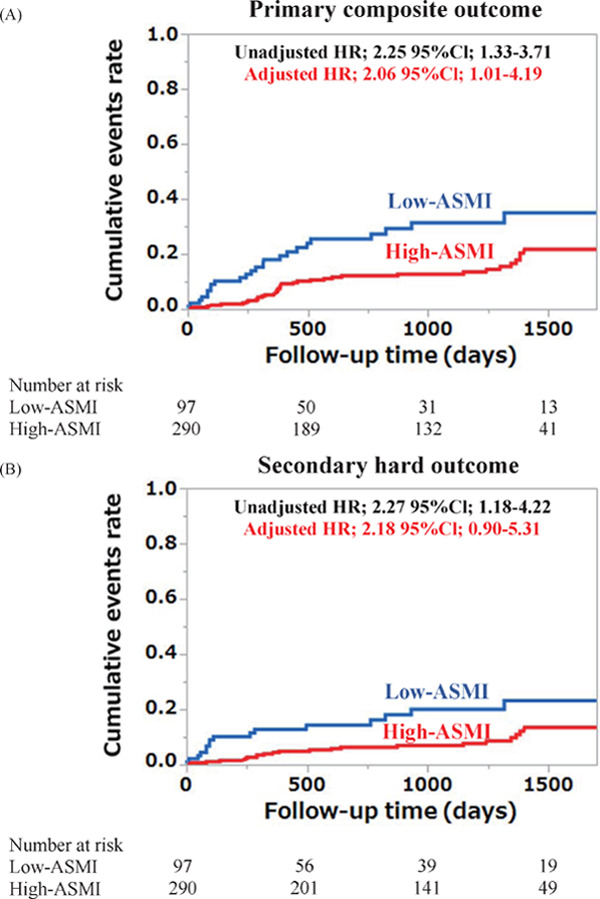
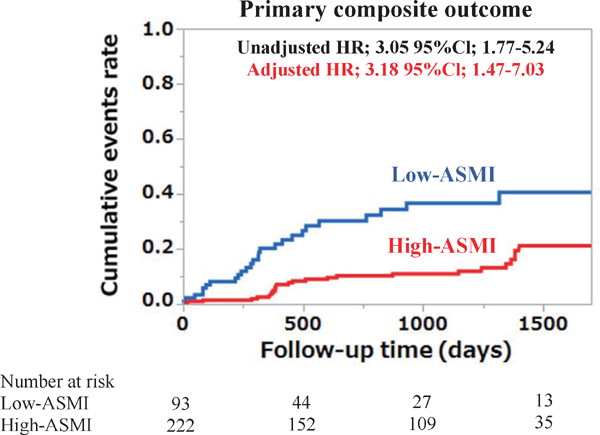
Methods: We measured SMM in 387 patients with STEMI using dual-energy X-ray absorptiometry. Patients were divided into low- and high-appendicular skeletal mass index (ASMI: appendicular SMM divided by height squared (kg/m2)) groups using the first quartile of ASMI (≤ 6.64 kg/m2 for men and ≤ 5.06 kg/m2 for women). All patients were followed up for the primary composite outcome of all-cause death, nonfatal myocardial infarction, nonfatal ischemic stroke, hospitalization for congestive heart failure, and unplanned revascularization.
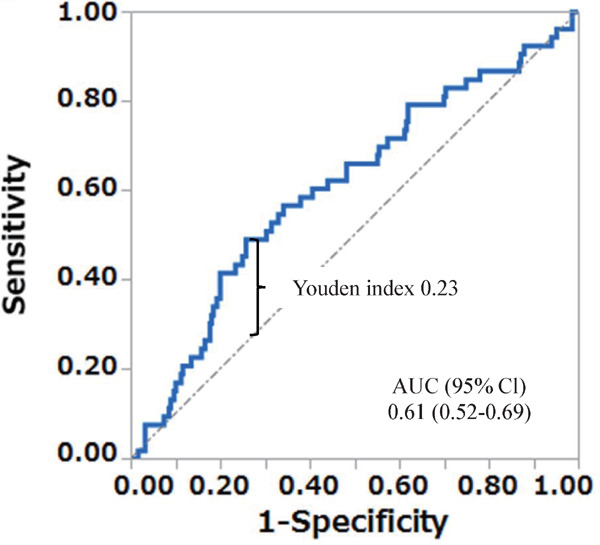
Results: Low-ASMI group was older and had a more complex coronary lesion, a lower left ventricular ejection fraction, and a higher prevalence of Killip classification ≥ 2 than high-ASMI group. During a median follow-up of 33 months, the event rate was significantly higher in low-ASMI group than in high-ASMI group (24.7% vs 13.4%, log-rank p=0.001). Even after adjustment for patients' background, low ASMI was independently associated with the high risk of primary composite events (adjusted hazard ratio 2.06, 95% confidence interval 1.01- 4.19, p=0.04). In the subgroup analyses of male patients (n=315), the optimal cutoff point of ASMI for predicting primary composite outcome was 6.75 kg/m2, which was close to its first quartile value.
Conclusions: Low ASMI is independently associated with poor outcome in patients with STEMI.
Keywords: ST-segment elevation myocardial infarction; Sarcopenia; Skeletal muscle mass.
Conflict of interest statement
Kiyoshi Hibi has been a paid consultant to or receiving fees for speaking from Daiichi-Sankyo, Terumo, Sanofi, Boston Scientific Japan, Amgen Astellas BioPharma, and Kowa Pharmaceutical. Stephan von Haehling has been a paid consultant to Vifor Pharma, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Brahms, Chugai Pharma, Roche, and Novartis. Stefan D. Anker has been a paid consultant to or receiving fees for speaking from Bayer, Boehringer Ingelheim, Thermo Fisher Scientific, Novartis, Servier, and Vifor Pharma; and his institution has received a research grant from Vifor Pharma and Abbott Vascular. Kazuo Kimura has been a paid consultant to or receiving fees for speaking from MSD, AstraZeneca, Daiichi-Sankyo and Bayer; and his institution has received a reserch grant from Kowa Pharmaceutical, Phyzer, MSD, Ono, Takeda, Eisai, Tanabe Mitsubishi, Daiichi-Sankyo, Bayer, AstraZeneca, Abbott Vascular Japan, Goodman, St. Jude Medical Japan, SOLVE, Teijin Pharma, and Medtronic Japan. Other authors declare that they have no conflicts of interest in the publication of this manuscript.
Figures
References
-
- Ryall JG, Schertzer JD, Lynch GS: Cellular and molecular mechanisms underlying age-related skeletal muscle wasting and weakness. Biogerontology, 2008; 9: 213-228 - PubMed
-
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M, European Working Group on Sarcopenia in Older P : Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing, 2010; 39: 412-423 - PMC - PubMed
-
- Kamiya K, Hamazaki N, Matsue Y, Mezzani A, Corra U, Matsuzawa R, Nozaki K, Tanaka S, Maekawa E, Noda C, Yamaoka-Tojo M, Matsunaga A, Masuda T, Ako J: Gait speed has comparable prognostic capability to six-minute walk distance in older patients with cardiovascular disease. Eur J Prev Cardiol, 2018; 25: 212-219 - PubMed
-
- Izawa KP, Watanabe S, Osada N, Kasahara Y, Yokoyama H, Hiraki K, Morio Y, Yoshioka S, Oka K, Omiya K: Handgrip strength as a predictor of prognosis in Japanese patients with congestive heart failure. Eur J Cardiovasc Prev Rehabil, 2009; 16: 21-27 - PubMed