

Closing the inequality gaps in reproductive, maternal, newborn and child health coverage: slow and fast progressors
- PMID: 32133181
- PMCID: PMC7042586
- DOI: 10.1136/bmjgh-2019-002230
Closing the inequality gaps in reproductive, maternal, newborn and child health coverage: slow and fast progressors
Abstract
Introduction: Universal Health Coverage (UHC) is a critical goal under the Sustainable Development Goals (SDGs) for health. Achieving this goal for reproductive, maternal, newborn and child health (RMNCH) service coverage will require an understanding of national progress and how socioeconomic and demographic subgroups of women and children are being reached by health interventions.
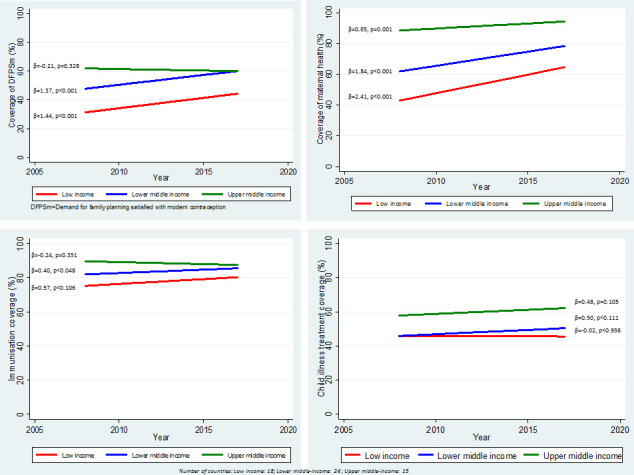
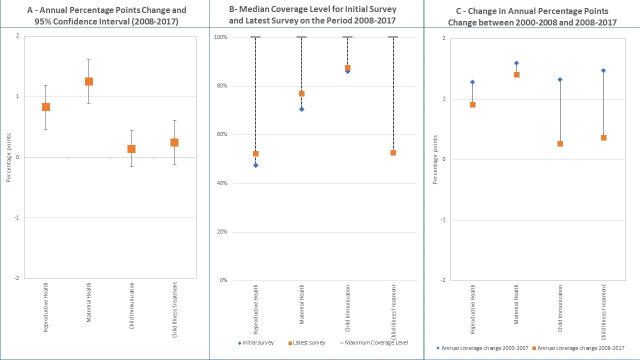
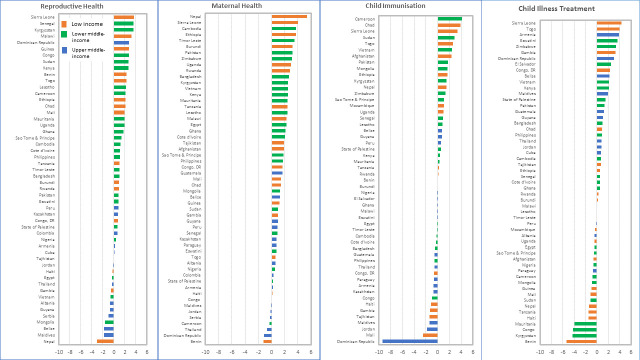
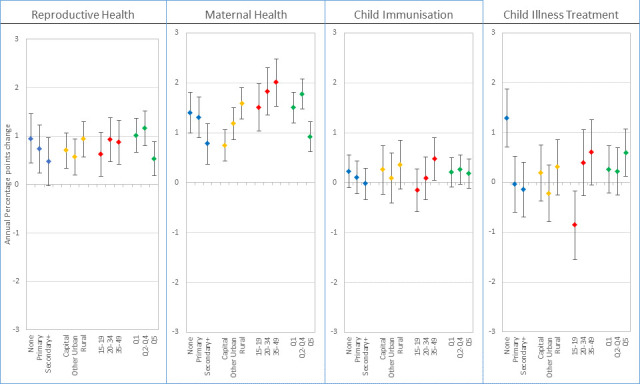
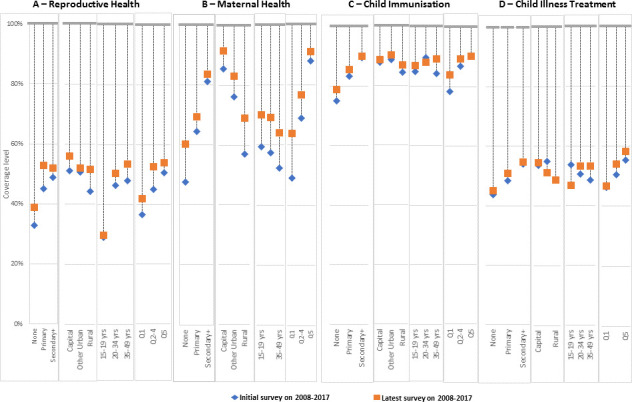
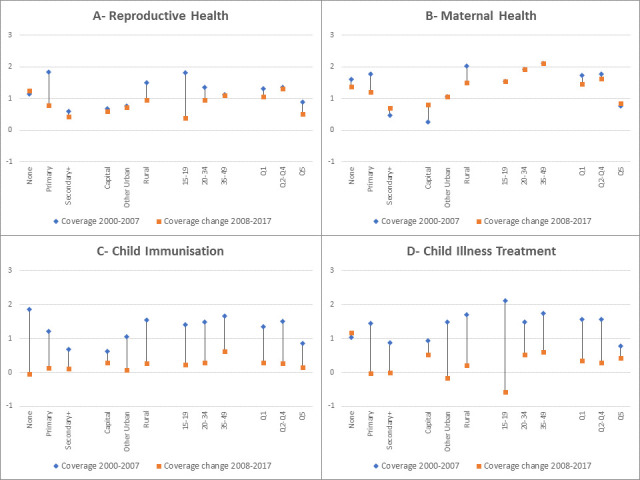
Methods: We accessed coverage databases produced by the International Centre for Equity in Health, which were based on reanalysis of Demographic and Health Surveys, Multiple Indicator Cluster Surveys and Reproductive and Health Surveys. We limited the data to 58 countries with at least two surveys since 2008. We fitted multilevel linear regressions of coverage of RMNCH, divided into four main components-reproductive health, maternal health, child immunisation and child illness treatment-to estimate the average annual percentage point change (AAPPC) in coverage for the period 2008-2017 across these countries and for subgroups defined by maternal age, education, place of residence and wealth quintiles. We also assessed change in the pace of coverage progress between the periods 2000-2008 and 2008-2017.
Results: Progress in RMNCH coverage has been modest over the past decade, with statistically significant AAPPC observed only for maternal health (1.25, 95% CI 0.90 to 1.61) and reproductive health (0.83, 95% CI 0.47 to 1.19). AAPPC was not statistically significant for child immunisation and illness treatment. Progress, however, varied largely across countries, with fast or slow progressors spread throughout the low-income and middle-income groups. For reproductive and maternal health, low-income and lower middle-income countries appear to have progressed faster than upper middle-income countries. For these two components, faster progress was also observed in older women and in traditionally less well-off groups such as non-educated women, those living in rural areas or belonging to the poorest or middle wealth quintiles than among groups that are well off. The latter groups however continue to maintain substantially higher coverage levels over the former. No acceleration in RMNCH coverage was observed when the periods 2000-2008 and 2008-2017 were compared.
Conclusion: At the dawn of the SDGs, progress in coverage in RMNCH remains insufficient at the national level and across equity dimensions to accelerate towards UHC by 2030. Greater attention must be paid to child immunisation to sustain the past gains and to child illness treatment to substantially raise its coverage across all groups.
Keywords: child health; maternal health.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- United Nations Transforming our world: the 2030 agenda for sustainable development, 2015. Available: https://sustainabledevelopment.un.org/content/documents/21252030%20Agend... [Accessed 27 Jul 2019].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous