

The CURE Protocol: evaluation and external validation of a new public health strategy for treating paediatric hydrocephalus in low-resource settings
- PMID: 32133193
- PMCID: PMC7042585
- DOI: 10.1136/bmjgh-2019-002100
The CURE Protocol: evaluation and external validation of a new public health strategy for treating paediatric hydrocephalus in low-resource settings
Abstract
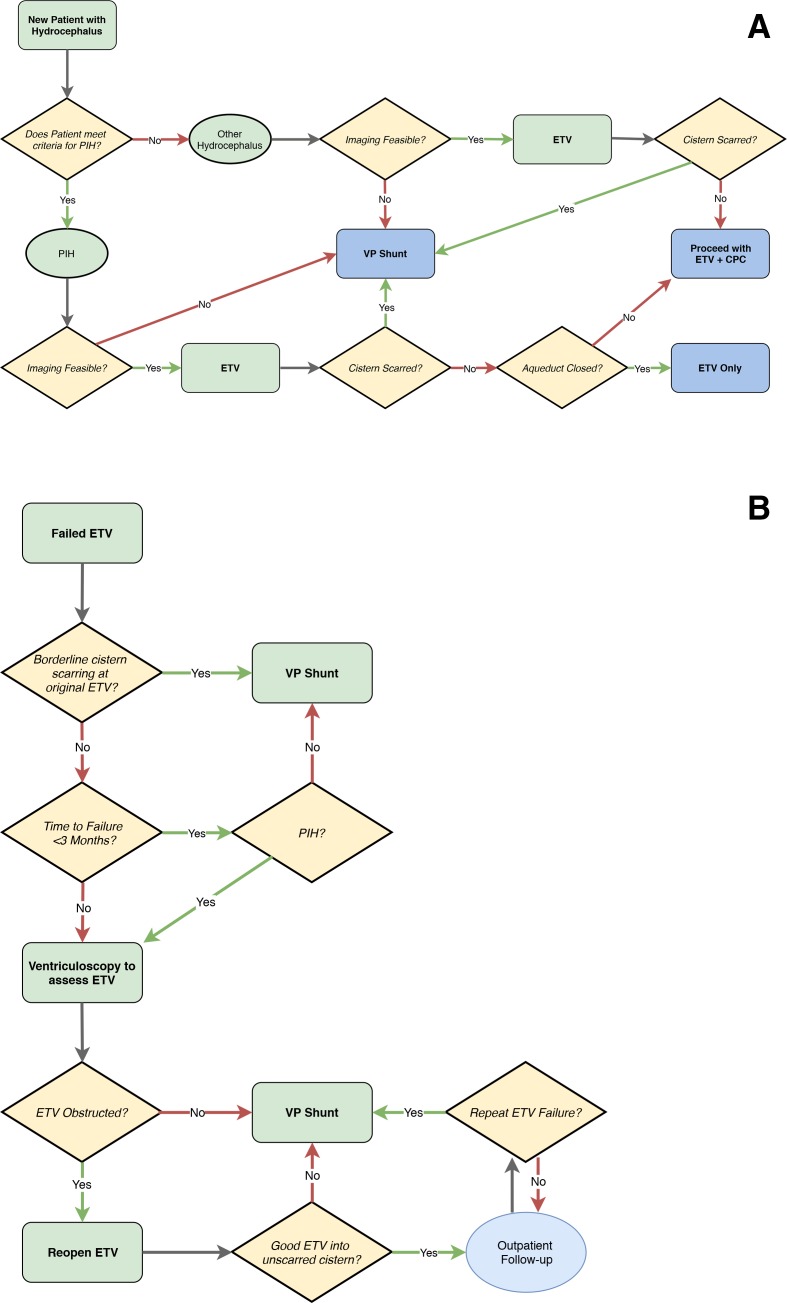
Introduction: Managing paediatric hydrocephalus with shunt placement is especially risky in resource-limited settings due to risks of infection and delayed life-threatening shunt obstruction. This study evaluated a new evidence-based treatment algorithm to reduce shunt-dependence in this context.
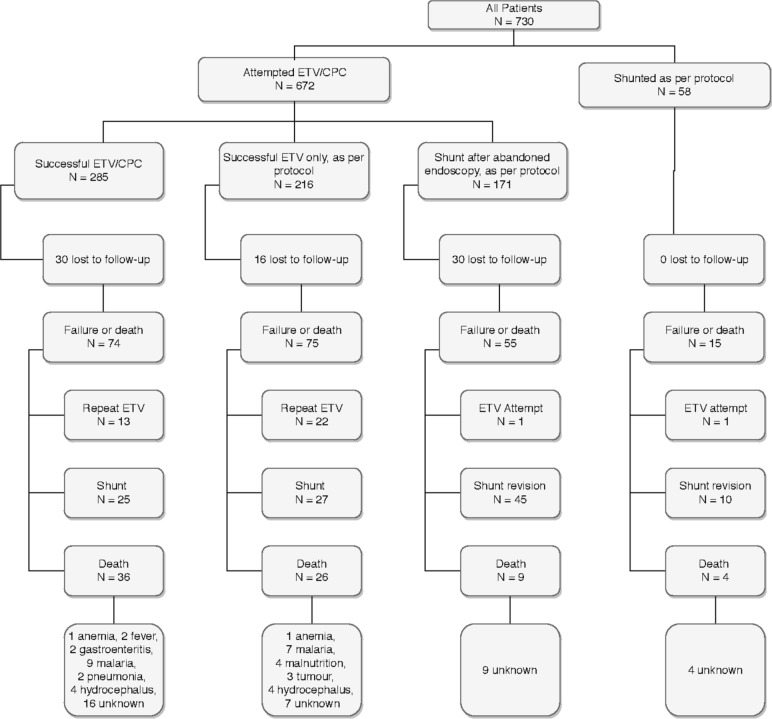
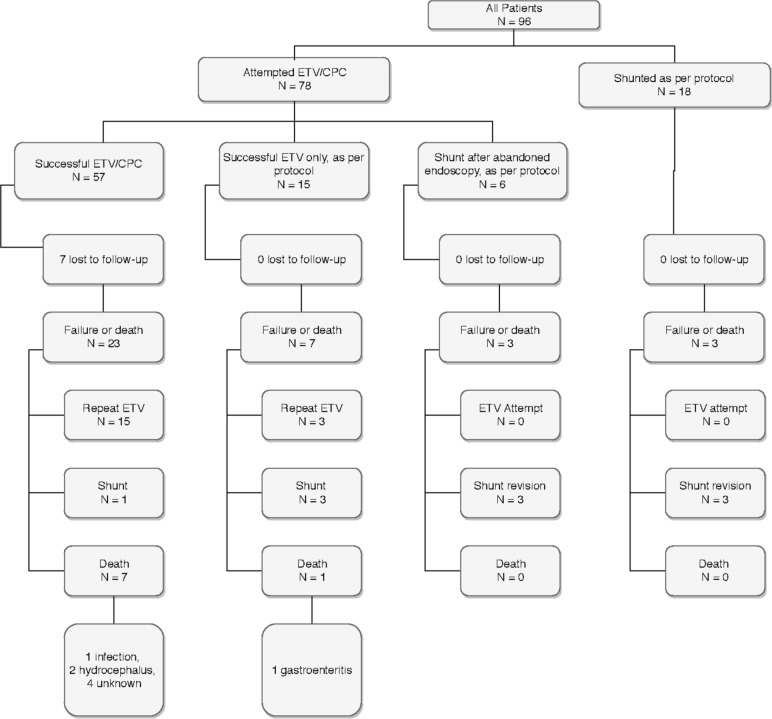
Methods: A prospective cohort design was used. The CURE Protocol employs preoperative and intraoperative data to choose between endoscopic treatment and shunt placement. Data were prospectively collected for 730 children in Uganda (managed by local neurosurgeons highly experienced in the protocol) and, for external validation, 96 children in Nigeria (managed by a local neurosurgeon trained in the protocol).
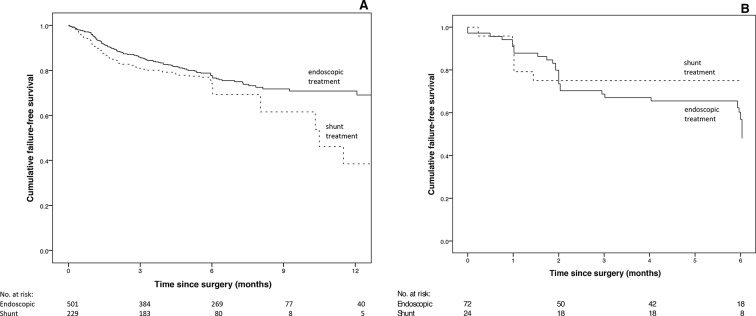
Results: The age distribution was similar between Uganda and Nigeria, but there were more cases of postinfectious hydrocephalus in Uganda (64.2% vs 26.0%, p<0.001). Initial treatment of hydrocephalus was similar at both centres and included either a shunt at first operation or endoscopic management without a shunt. The Nigerian cohort had a higher failure rate for endoscopic cases (adjusted HR 2.5 (95% CI 1.6 to 4.0), p<0.001), but not for shunt cases (adjusted HR 1.3 (0.5 to 3.0), p=0.6). Despite the difference in endoscopic failure rates, a similar proportion of the entire cohort was successfully treated without need for shunt at 6 months (55.2% in Nigeria vs 53.4% in Uganda, p=0.74).
Conclusion: Use of the CURE Protocol in two centres with different populations and surgeon experience yielded similar 6-month results, with over half of all children remaining shunt-free. Where feasible, this could represent a better public health strategy in low-resource settings than primary shunt placement.
Keywords: child health; cohort study; health education and promotion; health policy; meningitis.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Dewan MC, Rattani A, Mekary R, et al. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg 2018:1–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical