

Sequential Surgical Procedures in Vascular Surgery Patients Are Associated With Perioperative Adverse Cardiac Events
- PMID: 32133374
- PMCID: PMC7040239
- DOI: 10.3389/fcvm.2020.00013
Sequential Surgical Procedures in Vascular Surgery Patients Are Associated With Perioperative Adverse Cardiac Events
Abstract
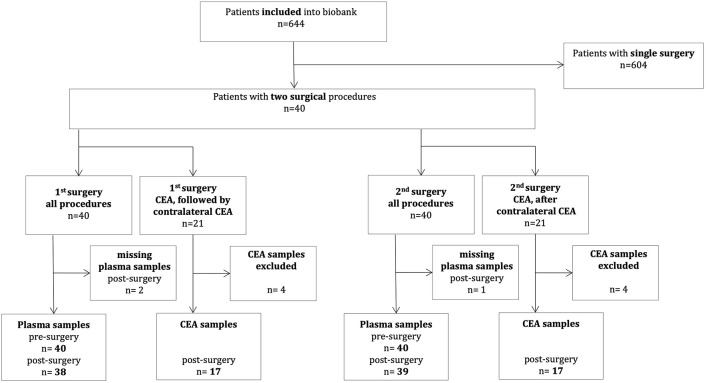
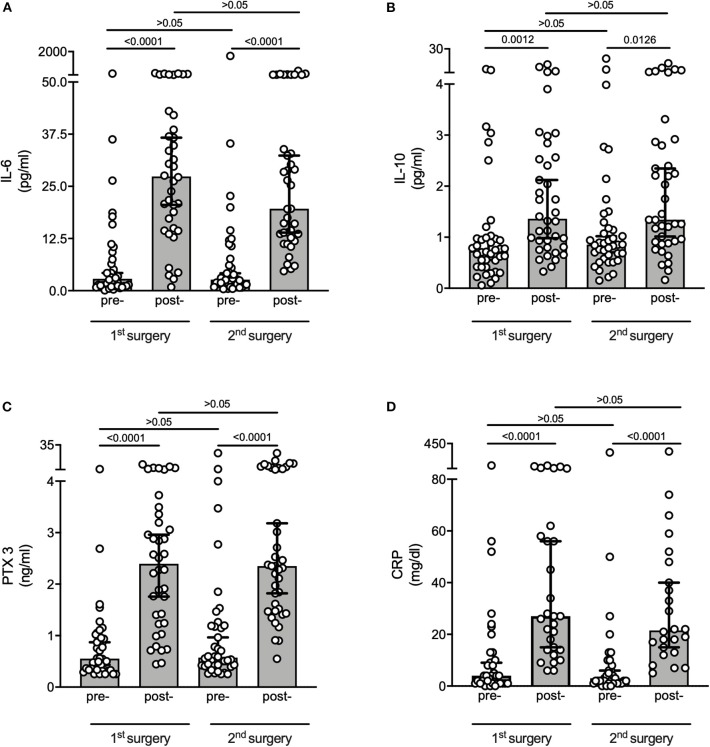
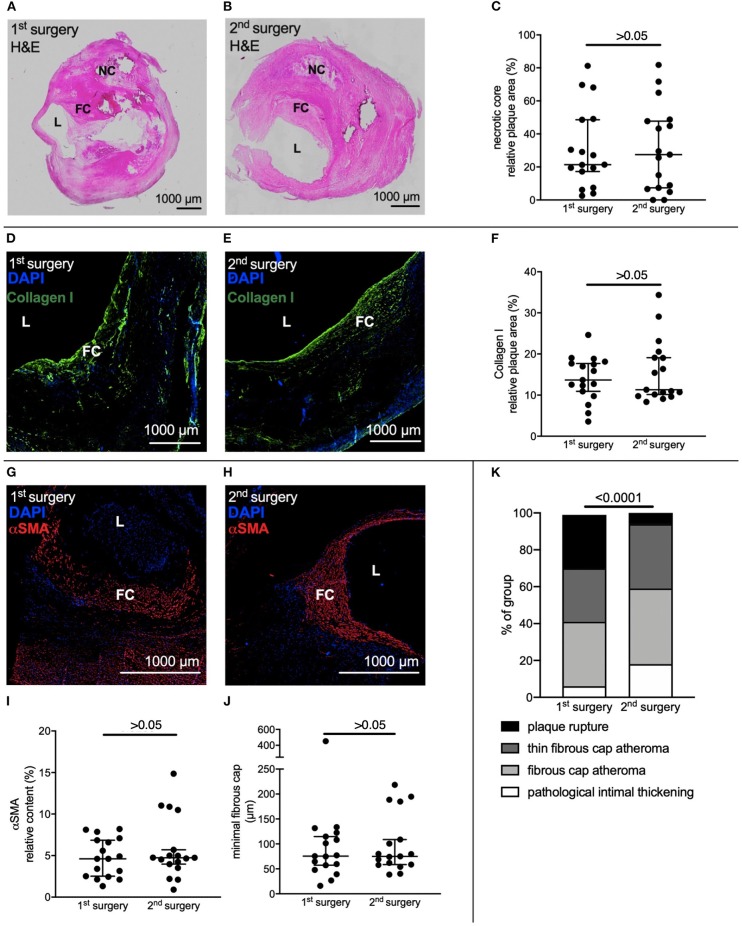
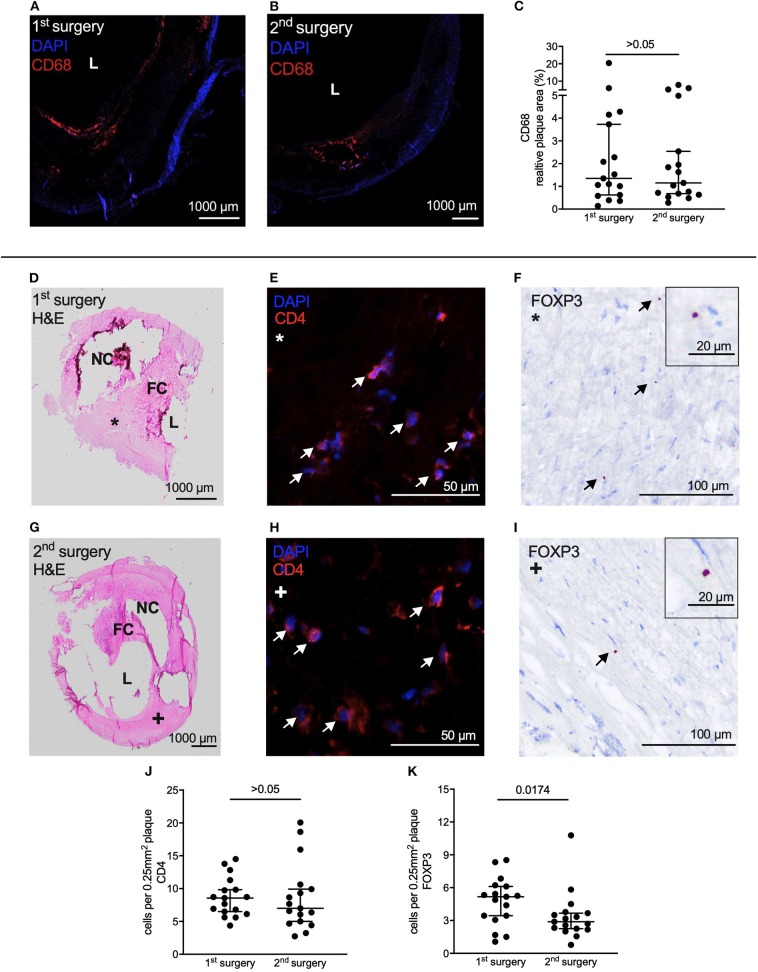
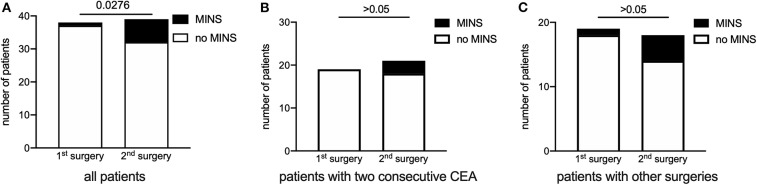
Patients at elevated cardiovascular risk are prone to perioperative cardiovascular complications, like myocardial injury after non-cardiac surgery (MINS). We have demonstrated in a mouse model of atherosclerosis that perioperative stress leads to an increase in plaque volume and higher plaque vulnerability. Regulatory T cells (Tregs) play a pivotal role in development and destabilization of atherosclerotic plaques. For this exploratory post-hoc analysis we identified 40 patients recruited into a prospective perioperative biomarker study, who within the inclusion period underwent sequential open vascular surgery. On the basis of protein markers measured in the biomarker study, we evaluated the perioperative inflammatory response in patients' plasma before and after index surgery as well as before and after a second surgical procedure. We also analyzed available immunohistochemistry samples to describe plaque vulnerability in patients who underwent bilateral carotid endarterectomy (CEA) in two subsequent surgical procedures. Finally, we assessed if MINS was associated with sequential surgery. The inflammatory response of both surgeries was characterized by postoperative increases of interleukin-6,-10, Pentraxin 3 and C-reactive protein with no clear-cut difference between the two time points of surgery. Plaques from CEA extracted during the second surgery contained less Tregs, as measured by Foxp3 staining, than plaques from the first intervention. The 2nd surgical procedure was associated with MINS. In conclusion, we provide descriptive evidence that sequential surgical procedures involve repeat inflammation, and we hypothesize that elevated rates of cardiovascular complications after the second procedure could be related to reduced levels of intraplaque Tregs, a finding that deserves confirmatory testing and mechanistic exploration in future populations.
Keywords: cardiac adverse event; interleukin-6; perioperative inflammation; plaque vulnerability; regulatory T cells; vascular surgery.
Copyright © 2020 Janssen, Felgner, Kummer, Gillmann, Schrimpf, Rustum, Lichtinghagen, Sahlmann, Weigand, Teebken, Theilmeier and Larmann.
Figures
References
-
- van Diepen S, Bakal JA, McAlister FA, Ezekowitz JA. Mortality and readmission of patients with heart failure, atrial fibrillation, or coronary artery disease undergoing noncardiac surgery: An analysis of 38 047 patients. Circulation. (2011) 124:289–96. 10.1161/CIRCULATIONAHA.110.011130 - DOI - PubMed
-
- Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, De Hert S, et al. 2014 esc/esa guidelines on non-cardiac surgery: cardiovascular assessment and management: the joint task force on non-cardiac surgery: cardiovascular assessment and management of the European society of cardiology (esc) and the european society of anaesthesiology (esa). Eur J Anaesthesiol. (2014) 31:517–73. 10.1097/EJA.0000000000000150 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials