

Where to look for the most frequent biases?
- PMID: 32133725
- PMCID: PMC7318122
- DOI: 10.1111/nep.13706
Where to look for the most frequent biases?
Abstract
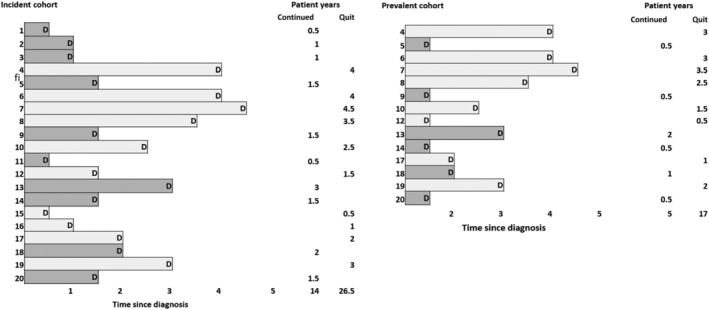
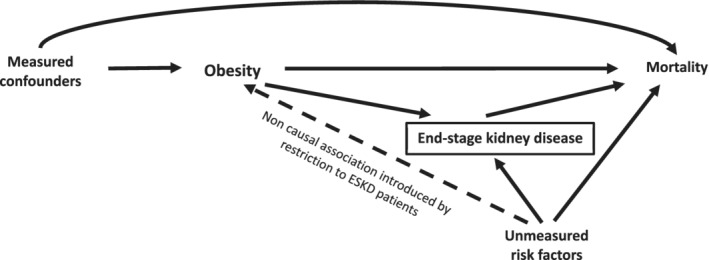
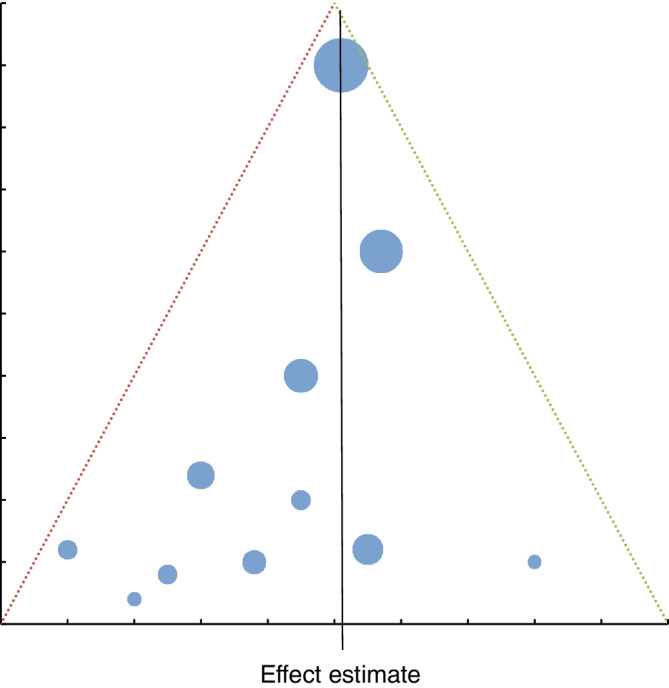
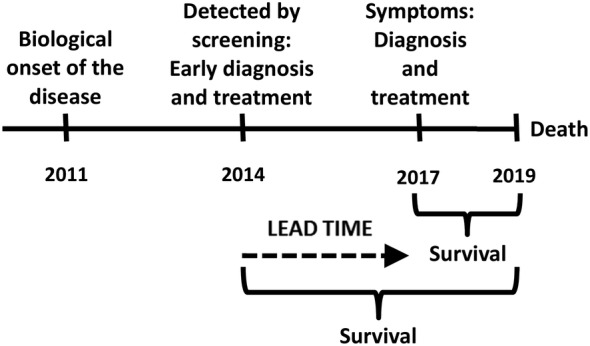
Study quality depends on a number of factors, one of them being internal validity. Such validity can be affected by random and systematic error, the latter also known as bias. Both make it more difficult to assess a correct frequency or the true relationship between exposure and outcome. Where random error can be addressed by increasing the sample size, a systematic error in the design, the conduct or the reporting of a study is more problematic. In this article, we will focus on bias, discuss different types of selection bias (sampling bias, confounding by indication, incidence-prevalence bias, attrition bias, collider stratification bias and publication bias) and information bias (recall bias, interviewer bias, observer bias and lead-time bias), indicate the type of studies where they most frequently occur and provide suggestions for their prevention.
Keywords: bias; epidemiologic methods; research design; research methodology.
© 2020 The Authors. Nephrology published by John Wiley & Sons Australia, Ltd on behalf of Asian Pacific Society of Nephrology.
Conflict of interest statement
We have no conflict of interest to report.
Figures
References
-
- Porta M, Greenland S, Hernãn S. In: Silva dos SI, Last M, eds. A dictionary of epidemiology. 6th ed. New York: Oxford University Press; 2014.
-
- Rothman KJ. Epidemiology. An Introduction, New York: Oxford University Press; 2002:20‐21.
-
- Catalogue of Bias Collaboration , Aronson JK, Bankhead C, Mahtani KR, Nunan D. Confounding by indication. In Catalogue of Biases. 2018. https://catalogofbias.org/biases/confounding-by-indication
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
