

Subcategorizing the Expected Value of Perfect Implementation to Identify When and Where to Invest in Implementation Initiatives
- PMID: 32133911
- PMCID: PMC7488812
- DOI: 10.1177/0272989X20907353
Subcategorizing the Expected Value of Perfect Implementation to Identify When and Where to Invest in Implementation Initiatives
Abstract
Purpose. Clinical practice variations and low implementation of effective and cost-effective health care technologies are a key challenge for health care systems and may lead to suboptimal treatment and health loss for patients. The purpose of this work was to subcategorize the expected value of perfect implementation (EVPIM) to enable estimation of the absolute and relative value of eliminating slow, low, and delayed implementation. Methods. Building on the EVPIM framework, this work defines EVPIM subcategories to estimate the expected value of eliminating slow, low, or delayed implementation. The work also shows how information on regional implementation patterns can be used to estimate the value of eliminating regional implementation variation. The application of this subcategorization is illustrated by a case study of the implementation of an antiplatelet therapy for the secondary prevention after myocardial infarction in Sweden. Incremental net benefit (INB) estimates are based on published cost-effectiveness assessments and a threshold of SEK 250,000 (£22,300) per quality-adjusted life year (QALY). Results. In the case study, slow, low, and delayed implementation was estimated to represent 22%, 34%, and 44% of the total population EVPIM (2941 QALYs or SEK 735 million), respectively. The value of eliminating implementation variation across health care regions was estimated to 39% of total EVPIM (1138 QALYs). Conclusion. Subcategorizing EVPIM estimates the absolute and relative value of eliminating different parts of suboptimal implementation. By doing so, this approach could help decision makers to identify which parts of suboptimal implementation are contributing most to total EVPIM and provide the basis for assessing the cost and benefit of implementation activities that may address these in future implementation of health care interventions.
Keywords: health care decision making; implementation strategies; value of implementation.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KMJ is a part-time PhD student at Linköping University and a part-time employee of Bristol Meyers Squibb AB, Sweden. The latter had no role in the present study. MH has no conflicts of interest. MJ received lecture fees from AstraZeneca and Pfizer. TJ received lecture fees from AstraZeneca, MSD, and Ipsen.
Figures
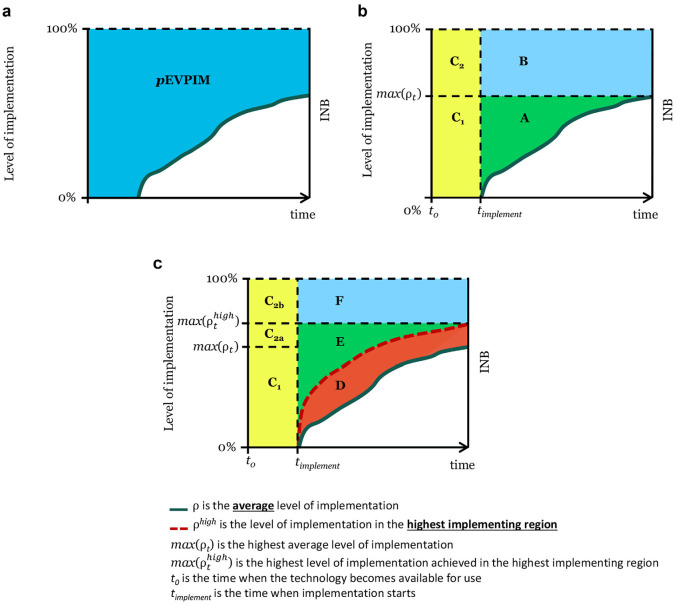
 ρ is the average level of implementation.
ρ is the average level of implementation.  ρhigh is the level of implementation in the highest implementing region. max(ρt) is the highest average level of implementation. max() is the highest level of implementation achieved in the highest implementing region. t0 is the time when the technology becomes available for use. timplement is the time when implementation starts.
ρhigh is the level of implementation in the highest implementing region. max(ρt) is the highest average level of implementation. max() is the highest level of implementation achieved in the highest implementing region. t0 is the time when the technology becomes available for use. timplement is the time when implementation starts.
Similar articles
-
Value of information and value of implementation: application of an analytic framework to inform resource allocation decisions in metastatic hormone-refractory prostate cancer.Value Health. 2009 Mar-Apr;12(2):315-24. doi: 10.1111/j.1524-4733.2008.00431.x. Epub 2008 Jul 24. Value Health. 2009. PMID: 18657098
-
Value of Implementation of Strategies to Increase the Adherence of Health Professionals and Cancer Survivors to Guideline-Based Physical Exercise.Value Health. 2017 Dec;20(10):1336-1344. doi: 10.1016/j.jval.2017.04.013. Epub 2017 Jun 20. Value Health. 2017. PMID: 29241893
-
How to Invest in Getting Cost-effective Technologies into Practice? A Framework for Value of Implementation Analysis Applied to Novel Oral Anticoagulants.Med Decis Making. 2017 Feb;37(2):148-161. doi: 10.1177/0272989X16645577. Epub 2016 Jul 10. Med Decis Making. 2017. PMID: 27105651
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
Quality-adjusted life-years lack quality in pediatric care: a critical review of published cost-utility studies in child health.Pediatrics. 2005 May;115(5):e600-14. doi: 10.1542/peds.2004-2127. Pediatrics. 2005. PMID: 15867026 Review.
Cited by
-
What methods are currently available for incorporating implementation considerations within the economic evaluation of health technologies? A scoping review.Health Res Policy Syst. 2024 Sep 30;22(1):134. doi: 10.1186/s12961-024-01220-9. Health Res Policy Syst. 2024. PMID: 39350148 Free PMC article.
-
The Value-of-Information and Value-of-Implementation from Clinical Trials of Diagnostic Tests for HIV-Associated Tuberculosis: A Modeling Analysis.MDM Policy Pract. 2023 Sep 22;8(2):23814683231198873. doi: 10.1177/23814683231198873. eCollection 2023 Jul-Dec. MDM Policy Pract. 2023. PMID: 37743931 Free PMC article.
-
Regional variation in prescription drug spending: Evidence from regional migrants in Sweden.Health Econ. 2022 Sep;31(9):1862-1877. doi: 10.1002/hec.4552. Epub 2022 Jun 16. Health Econ. 2022. PMID: 35709331 Free PMC article.
-
Cost-Effectiveness Analysis in Implementation Science: a Research Agenda and Call for Wider Application.Curr HIV/AIDS Rep. 2021 Jun;18(3):176-185. doi: 10.1007/s11904-021-00550-5. Epub 2021 Mar 20. Curr HIV/AIDS Rep. 2021. PMID: 33743138 Free PMC article. Review.
-
Implementation of Ticagrelor Reduced Mortality in Routine Clinical Care: Evidence From a Natural Experiment Including 109 995 Patients With Myocardial Infarction in Sweden.J Am Heart Assoc. 2023 Mar 7;12(5):e027384. doi: 10.1161/JAHA.122.027384. Epub 2023 Mar 4. J Am Heart Assoc. 2023. PMID: 36870964 Free PMC article.
References
-
- Mason J, Freemantle N, Nazareth I, Eccles M, Haines A, Drummond M. When is it cost-effective to change the behavior of health professionals? JAMA. 2001;286:2988–92. - PubMed
-
- Horton R. Public health research in the UK: the era of implementation. Lancet. 2015;386:1. - PubMed
-
- Karlsson LO, Nilsson S, Bång M, Nilsson L, Charitakis E, Janzon M. A clinical decision support tool for improving adherence to guidelines on anticoagulant therapy in patients with atrial fibrillation at risk of stroke: a cluster-randomized trial in a Swedish primary care setting (the CDS-AF study). PLoS Med. 2018;15:1–18. - PMC - PubMed
-
- Essat AM, Faria R, Gomersall T, et al. Getting Cost-Effective Technologies into Practice: The Value of Implementation. York, UK: University of York and University of Sheffield; 2013.
-
- Fenwick E, Claxton K, Sculpher M. The value of implementation and the value of information: combined and uneven development. Med Decis Making. 2008;28:21–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
