

Glycaemic status during pregnancy and longitudinal measures of fetal growth in a multi-racial US population: a prospective cohort study
- PMID: 32135135
- PMCID: PMC7676113
- DOI: 10.1016/S2213-8587(20)30024-3
Glycaemic status during pregnancy and longitudinal measures of fetal growth in a multi-racial US population: a prospective cohort study
Abstract
Background: The timepoint at which fetal growth begins to differ by maternal glycaemic status is not well understood. To address this lack of data, we examined gestational diabetes, impaired glucose tolerance, and early pregnancy glucose concentrations in relation to fetal growth trajectories.
Methods: This cohort study included 2458 pregnant women from the NICHD Fetal Growth Studies-Singletons study, which took place between 2009 and 2013. Women were recruited from 12 clinical centres in the USA. Women aged 18-40 years without major chronic conditions when entering pregnancy were included and those with records of neither glucose screening test or glucose tolerance test were excluded from the study. Women were enrolled at gestational weeks 8-13 and randomly assigned to four ultrasonogram schedules (Group A; weeks 16, 24, 30, 34; Group B: weeks 18, 26, 31, 35, 39; Group C: weeks 20, 28, 32, 36; Group D: weeks 22, 29, 33, 37, 41) to capture weekly fetal growth. Gestational diabetes, impaired glucose tolerance, and normal glucose tolerance were defined by medical record review. Glucose was measured in a subsample of women at weeks 10-14. We modelled fetal growth trajectories using linear mixed models with cubic splines. This study is registered with ClinicalTrials.gov, NCT00912132.
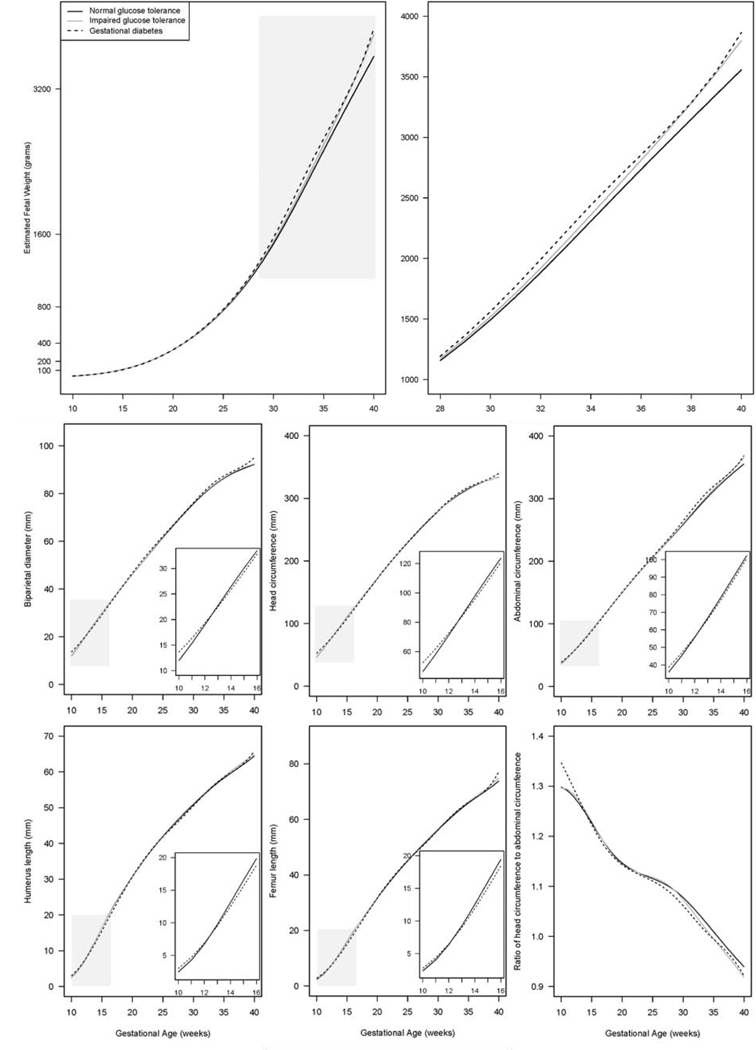
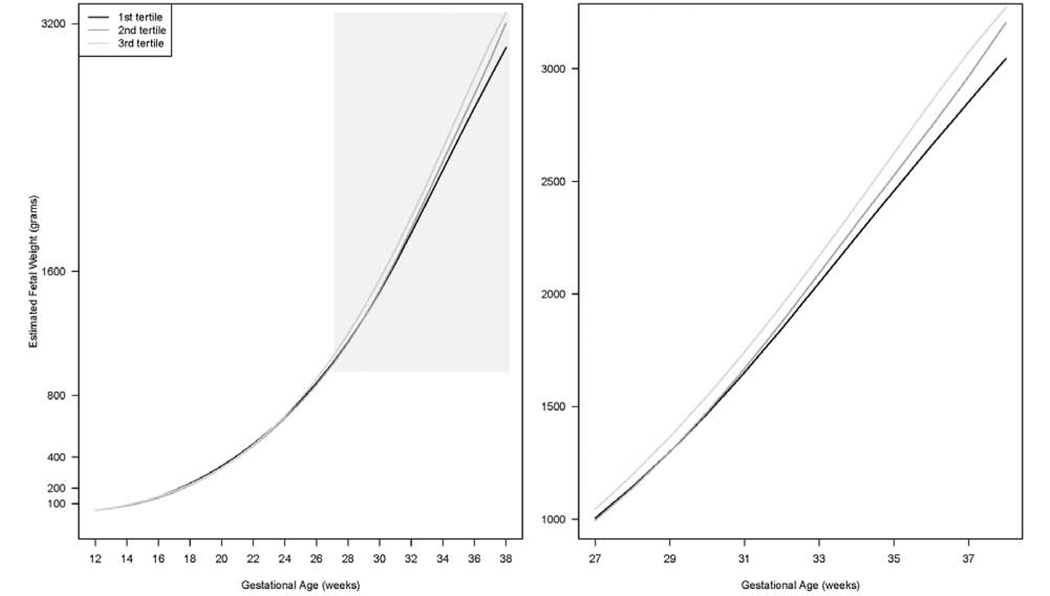
Findings: Of the 2458 women included in this study, 107 (4·4%) had gestational diabetes, 118 (4·8%) had impaired glucose tolerance, and 2020 (82·2%) had NGT. 213 women were excluded from the main analysis. The cohort with gestational diabetes was associated with a larger estimated fetal weight that started at week 20 and was significant at week 28-40 (at week 37: 3061 g [95% CI 2967-3164] for women with gestational diabetes vs 2943 g [2924-2962] for women with normal glucose tolerance, adjusted p=0·02). In addition, glucose levels at weeks 10-14 were positively associated with estimated fetal weight starting at week 23 and the association became significant at week 27 (at week 37: 3073 g [2983-3167] in the highest tertile vs 2853 g [2755-2955] in the lowest tertile, adjusted p=0·0009.
Interpretation: Gestational diabetes was associated with a larger fetal size that started at week 20 and became significant at gestational week 28. Efforts to mitigate gestational diabetes-related fetal overgrowth should start before 24-28 gestational weeks, when gestational diabetes is typically screened for in the USA.
Funding: National Institutes of Health.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Growing fat in utero: timing is everything.Lancet Diabetes Endocrinol. 2020 Apr;8(4):259-260. doi: 10.1016/S2213-8587(20)30064-4. Epub 2020 Mar 2. Lancet Diabetes Endocrinol. 2020. PMID: 32135133 No abstract available.
-
Gestational diabetes and fetal overgrowth: time to rethink screening guidelines.Lancet Diabetes Endocrinol. 2020 Jul;8(7):561-562. doi: 10.1016/S2213-8587(20)30189-3. Lancet Diabetes Endocrinol. 2020. PMID: 32559469 No abstract available.
Similar articles
-
Association of Maternal Obesity With Longitudinal Ultrasonographic Measures of Fetal Growth: Findings From the NICHD Fetal Growth Studies-Singletons.JAMA Pediatr. 2018 Jan 1;172(1):24-31. doi: 10.1001/jamapediatrics.2017.3785. JAMA Pediatr. 2018. PMID: 29131898 Free PMC article.
-
Racial/ethnic standards for fetal growth: the NICHD Fetal Growth Studies.Am J Obstet Gynecol. 2015 Oct;213(4):449.e1-449.e41. doi: 10.1016/j.ajog.2015.08.032. Am J Obstet Gynecol. 2015. PMID: 26410205 Free PMC article.
-
Plasma phospholipid polyunsaturated fatty acids composition in early pregnancy and fetal growth trajectories throughout pregnancy: Findings from the US fetal growth studies-singletons cohort.EBioMedicine. 2022 Aug;82:104180. doi: 10.1016/j.ebiom.2022.104180. Epub 2022 Jul 16. EBioMedicine. 2022. PMID: 35853297 Free PMC article. Clinical Trial.
-
Screening and diagnosing gestational diabetes mellitus.Evid Rep Technol Assess (Full Rep). 2012 Oct;(210):1-327. Evid Rep Technol Assess (Full Rep). 2012. PMID: 24423035 Free PMC article. Review.
-
Fetal biometry for guiding the medical management of women with gestational diabetes mellitus for improving maternal and perinatal health.Cochrane Database Syst Rev. 2019 Sep 3;9(9):CD012544. doi: 10.1002/14651858.CD012544.pub2. Cochrane Database Syst Rev. 2019. PMID: 31476798 Free PMC article.
Cited by
-
Trimester-specific reference intervals for hemoglobin A1c in non-diabetic pregnancy in a Chinese population.BMC Pregnancy Childbirth. 2023 Sep 19;23(1):671. doi: 10.1186/s12884-023-05980-0. BMC Pregnancy Childbirth. 2023. PMID: 37726666 Free PMC article.
-
Maternal Obesity Affects the Glucose-Insulin Axis During the First Trimester of Human Pregnancy.Front Endocrinol (Lausanne). 2020 Oct 9;11:566673. doi: 10.3389/fendo.2020.566673. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33154737 Free PMC article.
-
Maternal and neonatal outcomes of twin pregnancies complicated by gestational diabetes mellitus.Endocrine. 2024 May;84(2):388-398. doi: 10.1007/s12020-023-03588-0. Epub 2023 Nov 10. Endocrine. 2024. PMID: 37946069 Free PMC article.
-
Gestational Diabetes Mellitus and High Triglyceride Levels Mediate the Association between Pre-Pregnancy Overweight/Obesity and Macrosomia: A Prospective Cohort Study in Central China.Nutrients. 2022 Aug 16;14(16):3347. doi: 10.3390/nu14163347. Nutrients. 2022. PMID: 36014853 Free PMC article.
-
Assessing Glycemic Control Using CGM for Women with Diabetes in Pregnancy.Curr Diab Rep. 2021 Nov 4;21(11):44. doi: 10.1007/s11892-021-01415-2. Curr Diab Rep. 2021. PMID: 34735626 Review.
References
-
- HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. New England Journal of Medicine 2008; 358(19): 1991–2002. - PubMed
-
- McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nature reviews Disease primers 2019; 5(1): 47. - PubMed
-
- Sovio U, Murphy HR, Smith GC. Accelerated Fetal Growth Prior to Diagnosis of Gestational Diabetes Mellitus: A Prospective Cohort Study of Nulliparous Women. Diabetes care 2016; 39(6): 982–7. - PubMed
-
- Macaulay S, Munthali RJ, Dunger DB, Norris SA. The effects of gestational diabetes mellitus on fetal growth and neonatal birth measures in an African cohort. Diabetic medicine : a journal of the British Diabetic Association 2018; 35(10): 1425–33. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HHSN275201000001Z/HD/NICHD NIH HHS/United States
- HHSN275200800014C/HD/NICHD NIH HHS/United States
- HHSN275200800031C/HD/NICHD NIH HHS/United States
- HHSN275200800001C/HD/NICHD NIH HHS/United States
- HHSN275200800002C/HD/NICHD NIH HHS/United States
- HHSN275200800013C/HD/NICHD NIH HHS/United States
- HHSN275200800012C/HD/NICHD NIH HHS/United States
- HHSN275200800003I/HD/NICHD NIH HHS/United States
- HHSN27500006/HD/NICHD NIH HHS/United States
- HHSN275201000001G/HD/NICHD NIH HHS/United States
- HHSN275200800003C/HD/NICHD NIH HHS/United States
- HHSN275201000009C/HD/NICHD NIH HHS/United States
- HHSN275200800002I/HD/NICHD NIH HHS/United States
- HHSN275200800028C/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
