

Clinical implications with tolvaptan on monitored bioimpedance-defined fluid status in patients with cirrhotic ascites: an observational study
- PMID: 32138675
- PMCID: PMC7059268
- DOI: 10.1186/s12876-020-01205-2
Clinical implications with tolvaptan on monitored bioimpedance-defined fluid status in patients with cirrhotic ascites: an observational study
Abstract
Background: Prognostic value or clinical implications of fluid status monitoring in liver cirrhosis are not fully elucidated. Tolvaptan, an orally available, selective vasopressin V2-receptor antagonist approved for hyponatremia in the United States and European Union. It is also used for cirrhotic ascites at a relatively low dose (3.75 mg to 7.5 mg) in Japan, exerts its diuretic function by excreting electrolyte-free water. We hypothesized that bioimpedance-defined dynamic changes in fluid status allow prediction of response of V2 antagonism and survival in cirrhotic patients.
Methods: In this prospective observational study, 30 patients with decompensated liver cirrhosis who were unresponsive to conventional diuretics were enrolled. Detailed serial changes of body composition that were assessed by using non-invasive bioimpedance analysis (BIA) devices, along with biochemical studies, were monitored at 5 time points.
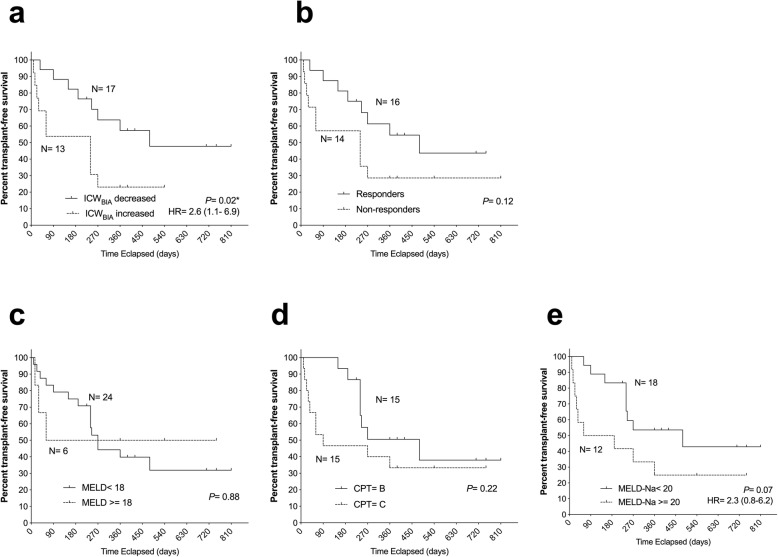
Results: Sixteen patients were classified as short-term responders (53%). Rapid and early decrease of BIA-defined intracellular water, as soon as 6 h after the first dose (ΔICWBIA%-6 h), significantly discriminated responders from non-responders (AUC = 0.97, P < 0.0001). ΔICWBIA%-6 h was highly correlated with the change of BIA-derived phase angle of trunk, e.g. reduced body reactance operated at 50 kHz after 24 h of the first dose of tolvaptan. Lower baseline blood urea nitrogen and lower serum aldosterone were predictive of a rapid and early decrease of ICWBIA. A rapid and early decrease of ICWBIA in response to tolvaptan was also predictive of a better transplant-free survival.
Conclusions: BIA-defined water compartment monitoring may help predict short-term efficacy and survival in decompensated cirrhotic patients treated with tolvaptan.
Keywords: Ascites; Impedance; Liver cirrhosis; Vasopressin antagonism.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Long-term administration of Tolvaptan to patients with decompensated cirrhosis.Int J Med Sci. 2020 Mar 15;17(7):874-880. doi: 10.7150/ijms.41454. eCollection 2020. Int J Med Sci. 2020. PMID: 32308540 Free PMC article.
-
Daily Monitoring of Serum Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein Is Useful for Predicting Therapeutic Effect of Tolvaptan in Cirrhotic Ascites.Tohoku J Exp Med. 2020 Dec;252(4):287-296. doi: 10.1620/tjem.252.287. Tohoku J Exp Med. 2020. PMID: 33208569
-
Impact of continued administration of tolvaptan on cirrhotic patients with ascites.BMC Pharmacol Toxicol. 2018 Dec 18;19(1):87. doi: 10.1186/s40360-018-0277-3. BMC Pharmacol Toxicol. 2018. PMID: 30563565 Free PMC article.
-
Tolvaptan for the treatment of liver cirrhosis oedema.Expert Rev Gastroenterol Hepatol. 2014 Jul;8(5):461-70. doi: 10.1586/17474124.2014.903797. Epub 2014 Mar 29. Expert Rev Gastroenterol Hepatol. 2014. PMID: 24678622 Review.
-
[Research progress of tolvaptan in the treatment of refractory ascites in cirrhosis].Zhonghua Gan Zang Bing Za Zhi. 2025 Jan 20;33(1):88-92. doi: 10.3760/cma.j.cn501113-20231225-00299. Epub 2024 Sep 3. Zhonghua Gan Zang Bing Za Zhi. 2025. PMID: 39929688 Review. Chinese.
Cited by
-
Consistency of the estimated target weights and ECW/TBW using BIA after hemodialysis in patients between standing and lying-down positions.BMC Nephrol. 2022 Mar 17;23(1):106. doi: 10.1186/s12882-022-02737-3. BMC Nephrol. 2022. PMID: 35300597 Free PMC article.
-
Management of Cirrhotic Ascites under the Add-on Administration of Tolvaptan.Int J Mol Sci. 2021 May 25;22(11):5582. doi: 10.3390/ijms22115582. Int J Mol Sci. 2021. PMID: 34070416 Free PMC article. Review.
-
The use of phase angle in patients with digestive and liver diseases.Rev Endocr Metab Disord. 2023 Jun;24(3):503-524. doi: 10.1007/s11154-023-09785-6. Epub 2023 Feb 6. Rev Endocr Metab Disord. 2023. PMID: 36745355 Review.
-
Bioelectrical Impedance Analysis (BIA) detects body resistance increase in dogs undergoing blood donation.Vet Res Commun. 2024 Dec;48(6):3889-3897. doi: 10.1007/s11259-024-10555-1. Epub 2024 Sep 27. Vet Res Commun. 2024. PMID: 39331344 Free PMC article.
References
-
- Collaborators GDIIP. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
-
- Lucena MI, Andrade RJ, Tognoni G, Hidalgo R, De La Cuesta FS. Spanish collaborative study group on therapeutic management in liver D. multicenter hospital study on prescribing patterns for prophylaxis and treatment of complications of cirrhosis. Eur J Clin Pharmacol. 2002;58(6):435–440. doi: 10.1007/s00228-002-0474-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
