

Stroke patients treated by thrombectomy in real life differ from cohorts of the clinical trials: a prospective observational study
- PMID: 32138684
- PMCID: PMC7059360
- DOI: 10.1186/s12883-020-01653-z
Stroke patients treated by thrombectomy in real life differ from cohorts of the clinical trials: a prospective observational study
Abstract
Background: Randomized controlled trials (RCTs) demonstrated efficacy and safety of endovascular treatment (ET) in anterior circulation large vessel occlusions (LVO). We aimed at investigating how stroke patients treated by thrombectomy in clinical practice and their outcome compare to cohorts and results of thrombectomy trials.
Methods: In a prospective study, we consecutively included stroke patients treated by thrombectomy (2015-2017). Baseline characteristics, procedural and outcome data were analyzed. Outcome was assessed by modified Rankin Scale (mRS) at 90 days. Ordinal regression analysis was performed to identify predictors of outcome.
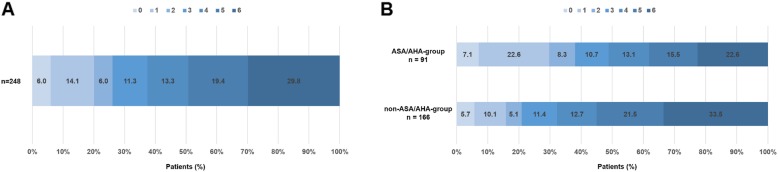
Results: Thrombectomy was applied in 264 patients (median 75 years, 49.6% female). Median baseline National Institutes of Health Stroke Scale (NIHSS) was 16, 58.0% received concomitant intravenous thrombolysis, 62.1% were referred from external hospitals. Median Alberta Stroke Program Early CT Score (ASPECTS) was 7. Successful recanalization (modified Thrombolysis in Cerebral Infarction Score, mTICI 2b/3) was achieved in 72.0%. Symptomatic intracranial hemorrhage (sICH) occurred in 4.5%. Independent outcome (mRS 0-2) was achieved in 26.2%, poor outcome (mRS 5-6) in 49.2%. Only 33.5% met the stringent enrolment criteria of previous RCTs. Lower age, baseline NIHSS, pre-stroke mRS, higher ASPECTS, and successful recanalization were independent predictors of favourable outcome.
Conclusions: The majority of stroke patients treated by ET in clinical practice would not have qualified for randomization in prior RCTs. Outcome in real-life patient cohorts is worse than in the highly selected cohorts from randomized trials, while rates of successful recanalization, sICH and outcome predictors are the same. Our findings support ET in broader patient populations than in the RCTs and may improve treatment decision in individual stroke patients with LVO in clinical practice.
Keywords: Basilar artery occlusion; Clinical practice; Reperfusion; Stroke; Thrombectomy.
Conflict of interest statement
MDC, HP, FF, HL and CB: The authors declare that they have no competing interests.
AA reports honoraria as speaker from Bayer Vital.
JF reports personal fees from Cerenovus, Penumbra, Route 92 Medical, grants and personal fees from Acandis, Medtronic, Microvention.
CG reports honoraria as speaker and/or scientific advisory board member from Actitor Biotech, Amgen, Bayer Healthcare, Boehringer Ingelheim, Prediction Biosciences, Sanofi Aventis.
GT7 reports personal fees from Acandis, grants and personal fees from Bayer, personal fees from Boehringer Ingelheim, personal fees from Bristol-Myers Squibb/Pfizer, personal fees from Daichi Sankyo, personal fees from Stryker, outside the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
