

Mediastinal paraganglioma successfully resected by robot-assisted thoracoscopic surgery with en bloc chest wall resection: a case report
- PMID: 32138719
- PMCID: PMC7057551
- DOI: 10.1186/s12893-020-00701-2
Mediastinal paraganglioma successfully resected by robot-assisted thoracoscopic surgery with en bloc chest wall resection: a case report
Abstract
Background: Robot-assisted thoracoscopic surgery (RATS) is useful for surgery in the apical region of the chest cavity, as it narrows towards the head. Here, we describe a nonfunctional, rib-invasive paraganglioma arising in the posterior mediastinum that was successfully removed using RATS combined with chest wall resection.
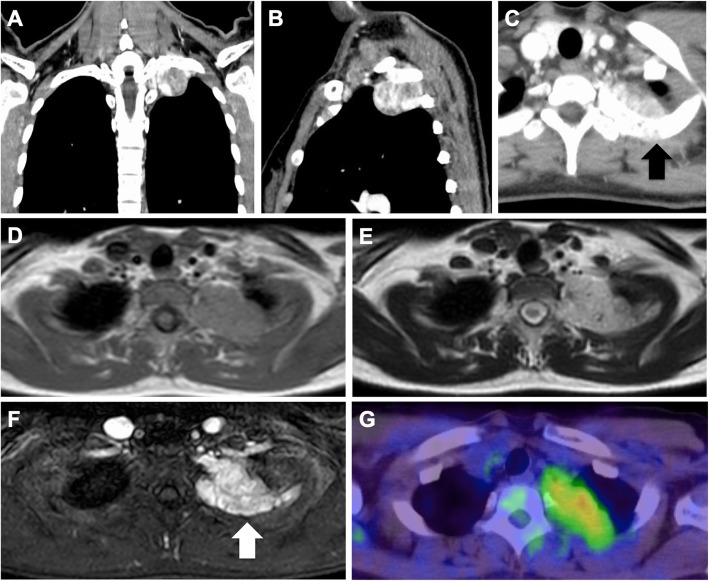
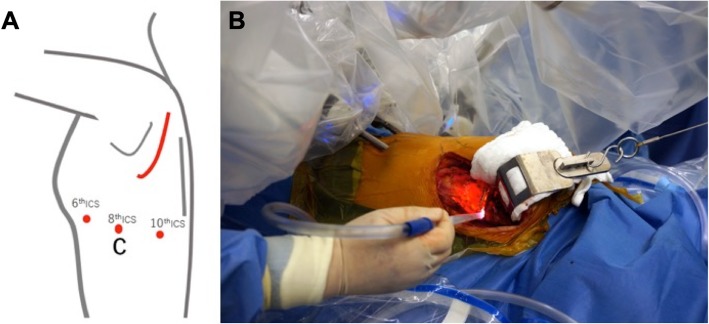
Case presentation: A 31-year-old woman presented with a posterior mediastinal mass on chest computed tomography (CT) scan during a medical check-up 2 years prior. Positron emission tomography/computed tomography scan with F-18 fluorodeoxyglucose revealed a mass associated with standardized uptake maximum value of 2.69. With a preoperative diagnosis of neurogenic tumor by CT-guided percutaneous fine-needle aspiration biopsy, we performed robot-assisted tumor resection combined with chest wall resection. The wristed instruments of the robotic surgical system have increased range of motion and enabled the tumor resection without organ injury in the thoracic cavity. Histopathology examination revealed a non-functional paraganglioma with rib invasion.
Conclusions: RATS is a useful technique, enabling safer and easier resection of a mediastinal tumor adjacent to surrounding organs.
Keywords: Mediastinal tumor; Paraganglioma; Robot-assisted thoracoscopic surgery.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Homma T, Kitamura N, Ojima T, Akemoto Y, Hida Y, Yoshimura N. Initial experiences of robot-assisted thoracic surgery: safety approach and comparison with video-assisted thoracoscopic surgery. Jpn J Chest Surg. 2019;33(2):113–121. doi: 10.2995/jacsurg.33.113. - DOI
-
- Takaji K, Yoshioka M, Mori T, Tsuruzoe S, Tabira Y, Tanaka M, et al. A case of schwannomaarising in brachial plexus with intrathoracic extension. Jpn J Chest Surg. 1999;13(5):700–704. doi: 10.2995/jacsurg.13.700. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
