

Paracrine and cell autonomous signalling in pancreatic cancer progression and metastasis
- PMID: 32139180
- PMCID: PMC7118576
- DOI: 10.1016/j.ebiom.2020.102662
Paracrine and cell autonomous signalling in pancreatic cancer progression and metastasis
Abstract
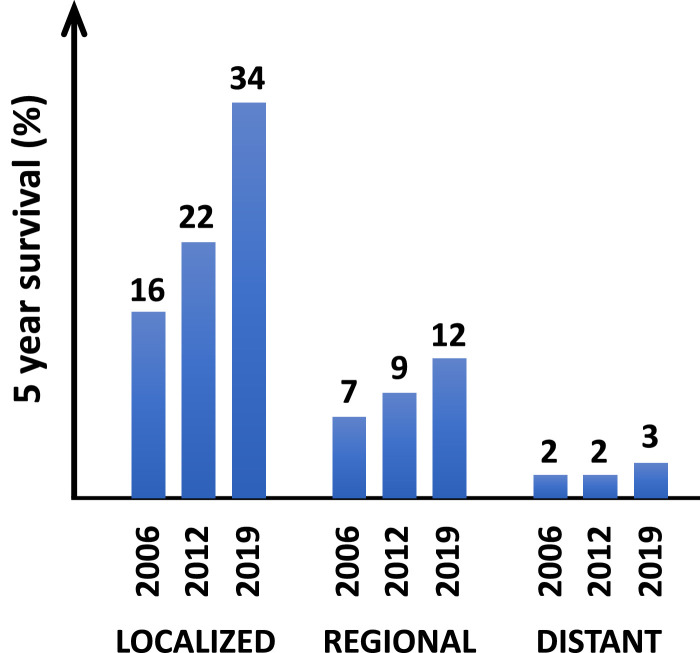
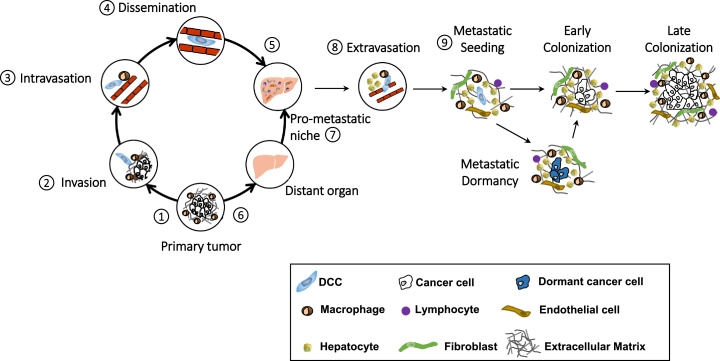
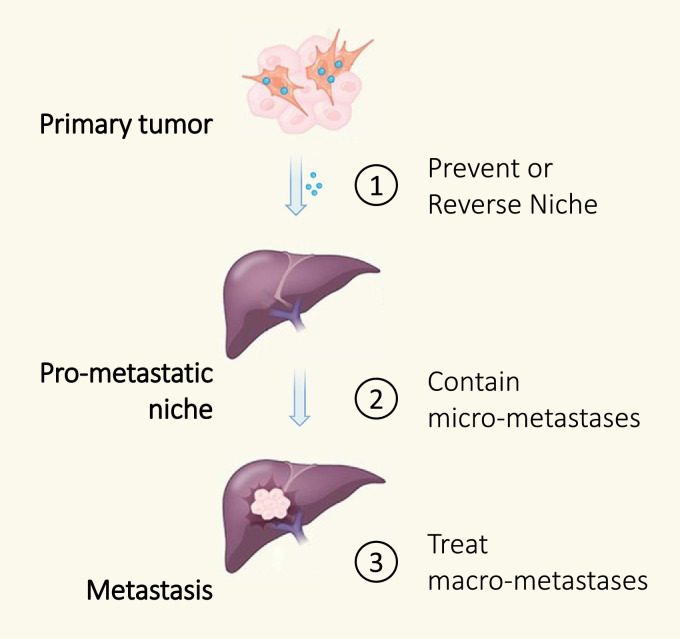
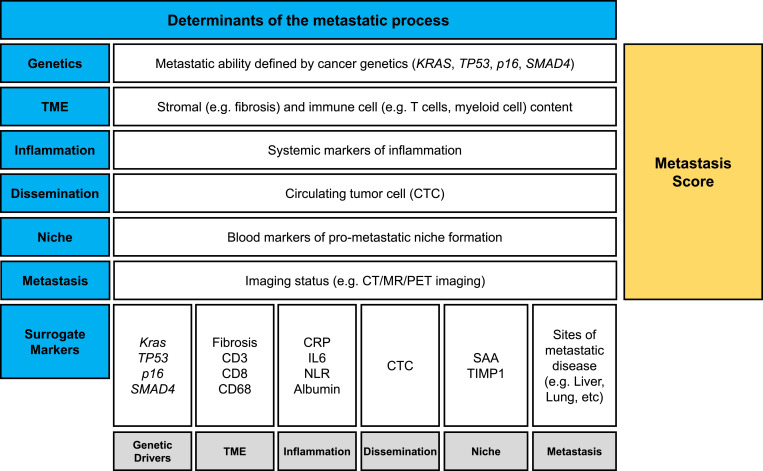
Pancreatic ductal adenocarcinoma (PDAC) shows remarkable propensity to metastasize. This predilection to escape from the primary tumor is driven by paracrine and autocrine mechanisms that guide cancer cells through a multi-step process concluding with colonization in distant tissues. Although cell-intrinsic features support the metastatic ability of cancer cells, permissive microenvironments within the primary organ and at sites of distant metastasis may be rate-limiting. Identification of cancer cell-extrinsic factors that regulate formation of these environments lend new therapeutic targets for intervening on the metastatic cascade. In addition, the bipolar, yet fundamental, role of the immune system in the metastatic process presents therapeutic opportunities. Herein, we review the current knowledge of the metastatic cascade in PDAC, and propose that genomically stable determinants of metastasis (e.g. the pro-metastatic niche and immune system) are actionable targets for preventing, containing, and treating metastasis in PDAC.
Keywords: Cancer; Clinical trials; Immune evasion; Immunosurveillance; Immunotherapy; Inflammation; Macrophages; Metastasis; Neutrophils; Pancreatic ductal adenocarcinoma; T cells; Therapeutic resistance; Treatment paradigms; Tumor microenvironment; Vaccines.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest G.L.B. is a consultant/advisory board member for Seattle Genetics, Aduro Biotech, AstraZeneca, Bristol-Myers Squibb, Incyte, Genmab, Takeda, Merck, and BiolineRx; reports receiving commercial research grants from Incyte, Bristol-Myers Squibb, Verastem, Halozyme, Biothera, Arcus, Newlink, Novartis, and Janssen; and is an inventor of intellectual property and recipient of royalties from Novartis and Advaxis, Inc. No potential conflicts of interest were disclosed by the other authors.
Figures
Comment in
-
Working together to reduce the burden of pancreatic cancer.Lancet Oncol. 2020 Mar;21(3):334-335. doi: 10.1016/S1470-2045(20)30088-7. Lancet Oncol. 2020. PMID: 32135099 No abstract available.
References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Rahib L., Smith B.D., Aizenberg R., Rosenzweig A.B., Fleshman J.M., Matrisian L.M. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. - PubMed
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362(17):1605–1617. - PubMed
-
- Sperti C., Pasquali C., Piccoli A., Pedrazzoli S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg. 1997;21(2):195–200. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
