

Patterns and predictors of co-morbidities in Tuberculosis: A cross-sectional study in the Philippines
- PMID: 32139742
- PMCID: PMC7058028
- DOI: 10.1038/s41598-020-60942-2
Patterns and predictors of co-morbidities in Tuberculosis: A cross-sectional study in the Philippines
Abstract
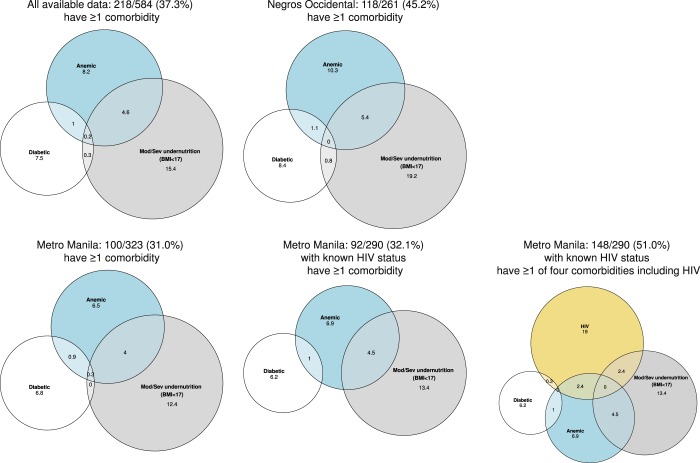
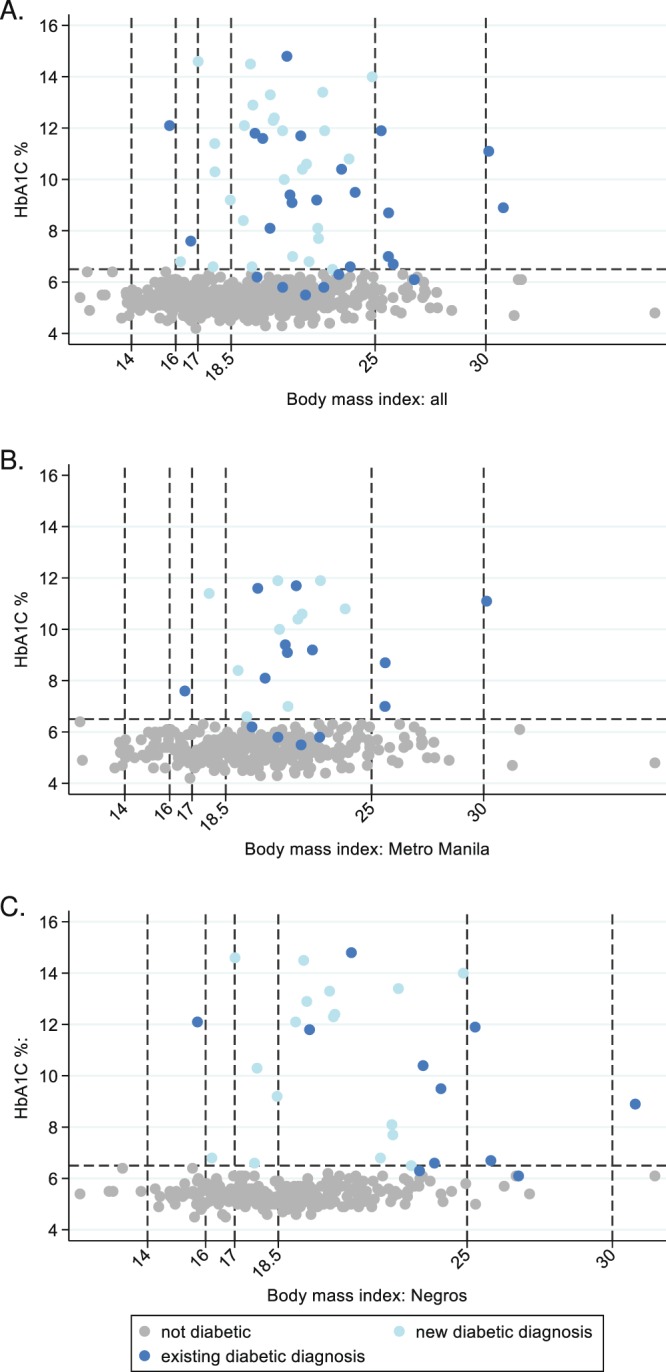
Diabetes and undernutrition are common risk factors for TB, associated with poor treatment outcomes and exacerbated by TB. We aimed to assess non-communicable multimorbidity (co-occurrence of two or more medical conditions) in Filipino TB outpatients, focusing on malnutrition and diabetes. In a cross-sectional study, 637 adults (70% male) from clinics in urban Metro Manila (N = 338) and rural Negros Occidental (N = 299) were enrolled. Diabetes was defined as HbA1c of ≥6.5% and/or current diabetes medication. Study-specific HIV screening was conducted. The prevalence of diabetes was 9.2% (54/589, 95%CI: 7.0-11.8%) with 52% newly diagnosed. Moderate/severe undernutrition (body mass index (BMI) <17 kg/2) was 20.5% (130/634, 95%CI: 17.4-23.9%). Forty percent of participants had at least one co-morbidity (diabetes, moderate/severe undernutrition or moderate/severe anaemia (haemoglobin <11 g/dL)). HIV infection (24.4%, 74/303) was not associated with other co-morbidities (but high refusal in rural clinics). Central obesity assessed by waist-to-hip ratio was more strongly associated with diabetes (Adjusted Odds Ratio (AOR) = 6.16, 95%CI: 3.15-12.0) than BMI. Undernutrition was less common in men (AOR = 0.44, 95%CI: 0.28-0.70), and associated with previous history of TB (AOR = 1.97, 95%CI: 1.28-3.04) and recent reduced food intake. The prevalence of multimorbidity was high demonstrating a significant unmet need. HIV was not a risk factor for increased non-communicable multimorbidity.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO. Global TB Report. (2019).
