

Efficacy and Safety of a Pressurized Metered-Dose Inhaler in Older Asthmatics: Comparison to a Dry Powder Inhaler in a 12-Week Randomized Trial
- PMID: 32141259
- PMCID: PMC7061154
- DOI: 10.4168/aair.2020.12.3.454
Efficacy and Safety of a Pressurized Metered-Dose Inhaler in Older Asthmatics: Comparison to a Dry Powder Inhaler in a 12-Week Randomized Trial
Abstract
Purpose: Asthma control in older asthmatics is often less effective, which may be attributed to small airway dysfunction and poor inhalation technique. We compared the efficacy of 2 inhalers (fluticasone propionate/formoterol treatment using a pressurized metered-dose inhaler [p-MDI group] vs. fluticasone propionate/salmeterol treatment using a dry powder inhaler [DPI group]) in older asthmatics.
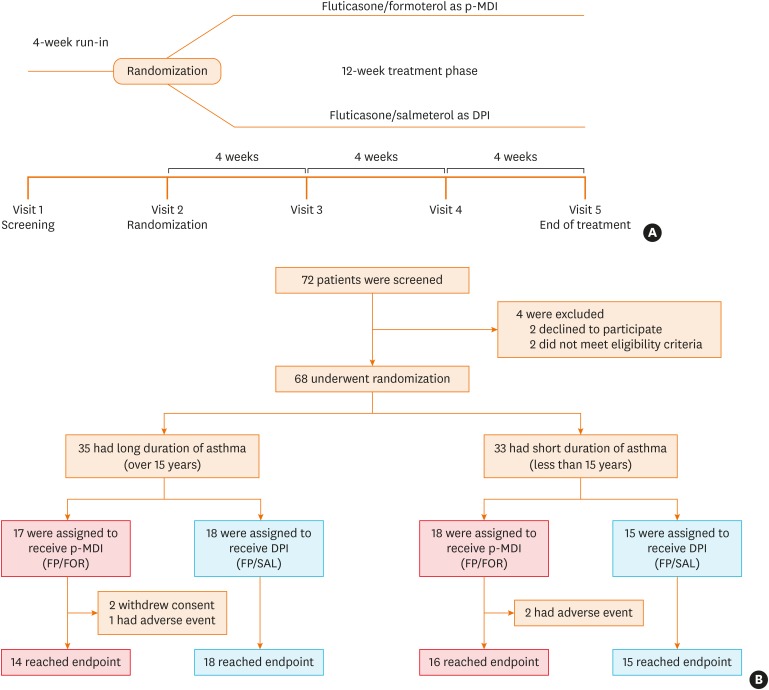
Methods: We conducted a 12-week, randomized, open-label, parallel-designed trial in older patients (over 55 years old) with moderate-to-severe asthma, and compared the efficacy and safety for asthma control between the 2 groups. Subgroup analyses on disease duration and air trapping were performed. Clinical parameters, including changes in lung function parameters, inhaler technique and adherence, were compared with monitoring adverse reactions between the 2 groups.
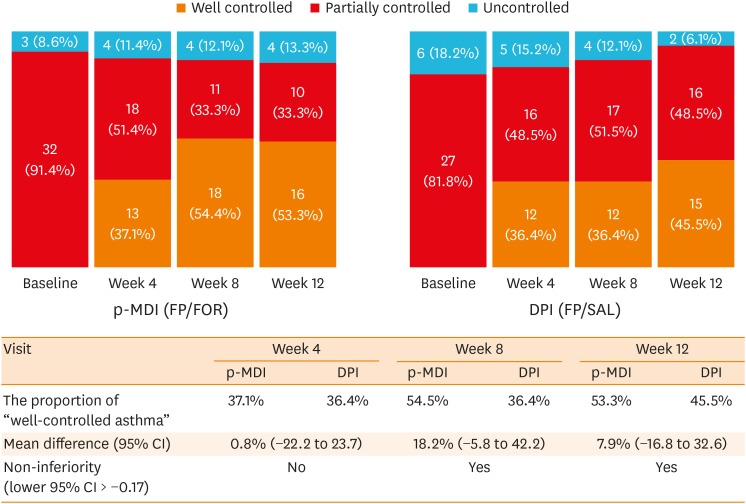
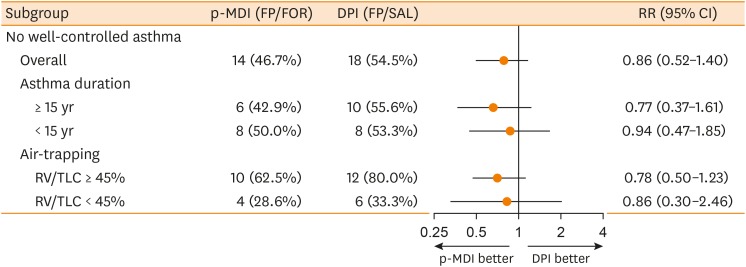
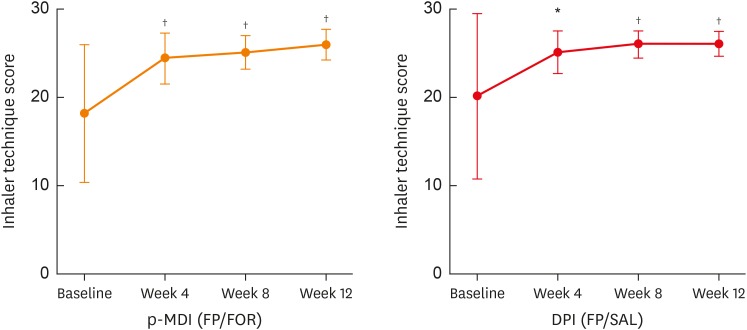
Results: A total of 68 patients underwent randomization, and 63 (30 in the p-MDI group and 33 in the DPI group) completed this study. The p-MDI group was non-inferior to the DPI group with regard to the rate of well-controlled asthma (53.3% vs. 45.5%, p < 0.001; a predefined non-inferiority limit of 17%). In subgroup analyses, the proportion of patients who did not reach well-controlled asthma in the p-MDI group was non-inferior to that in the DPI group; the difference was 12.7% among those with a longer disease duration (≥ 15 years) and 17.5% among those with higher air-trapping (RV/TLC ≥ 45%), respectively (a predefined non-inferiority limit of 17%, p < 0.001). No significant differences were observed in lung function parameters, inhalation techniques, adherence and adverse reactions between the 2 groups.
Conclusion: These results suggest that the p-MDI group may be comparable to the DPI group in the management of older asthmatics in aspects of efficacy and safety.
Keywords: Asthma; aged; airway management; dry powder inhalers; medication adherence; metered dose inhalers.
Copyright © 2020 The Korean Academy of Asthma, Allergy and Clinical Immunology · The Korean Academy of Pediatric Allergy and Respiratory Disease.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interests.
Figures
References
-
- Gibson PG, McDonald VM, Marks GB. Asthma in older adults. Lancet. 2010;376:803–813. - PubMed
-
- Niewoehner DE, Kleinerman J. Morphologic basis of pulmonary resistance in the human lung and effects of aging. J Appl Physiol. 1974;36:412–418. - PubMed
-
- Milic-Emili J, Torchio R, D'Angelo E. Closing volume: a reappraisal (1967–2007) Eur J Appl Physiol. 2007;99:567–583. - PubMed
-
- Janssens JP, Pache JC, Nicod LP. Physiological changes in respiratory function associated with ageing. Eur Respir J. 1999;13:197–205. - PubMed
