

Increasing Prevalence and Mortality of Asthma With Age in Korea, 2002-2015: A Nationwide, Population-Based Study
- PMID: 32141260
- PMCID: PMC7061163
- DOI: 10.4168/aair.2020.12.3.467
Increasing Prevalence and Mortality of Asthma With Age in Korea, 2002-2015: A Nationwide, Population-Based Study
Abstract
Purpose: The prevalence of asthma is increasing globally as the world population increases; however, and the prevalence and mortality of asthma have not been extensively investigated. Also, the effects of severity and aging on asthma prevalence and mortality are unknown. We aimed to investigate trends of the prevalence and mortality of asthma as well as health care uses and costs over 14 years according to disease severity by using real-world data in Korea.
Methods: Using the National Health Insurance Sharing Service database, we extracted asthmatic patients having diagnosis codes of asthma and prescription records of antiasthmatic medications from 2002 to 2015 and categorized them according to asthma exacerbation and regular treatment. We defined asthma-associated death in terms of patients' prescription records within 3 months before all-cause death, then linked with the Cause of Death Statistics. The annual asthma-related health care uses and costs were analyzed.
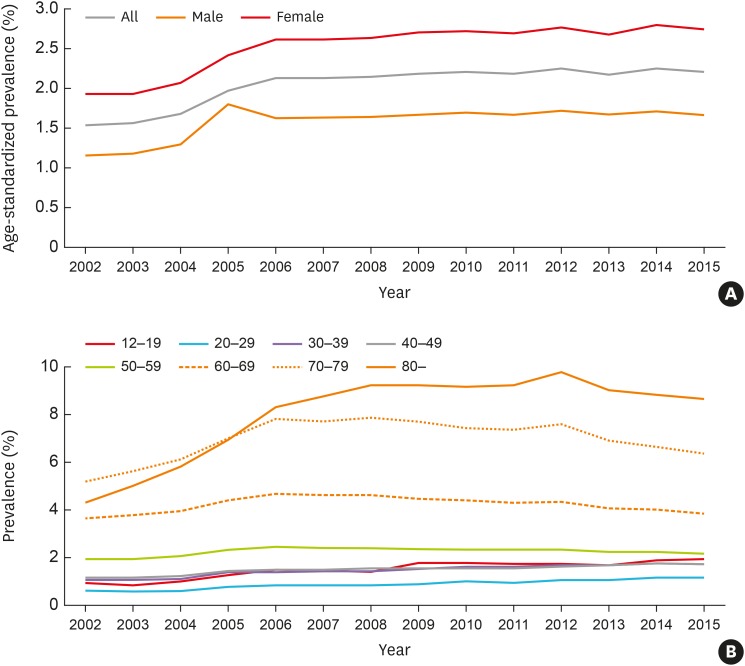
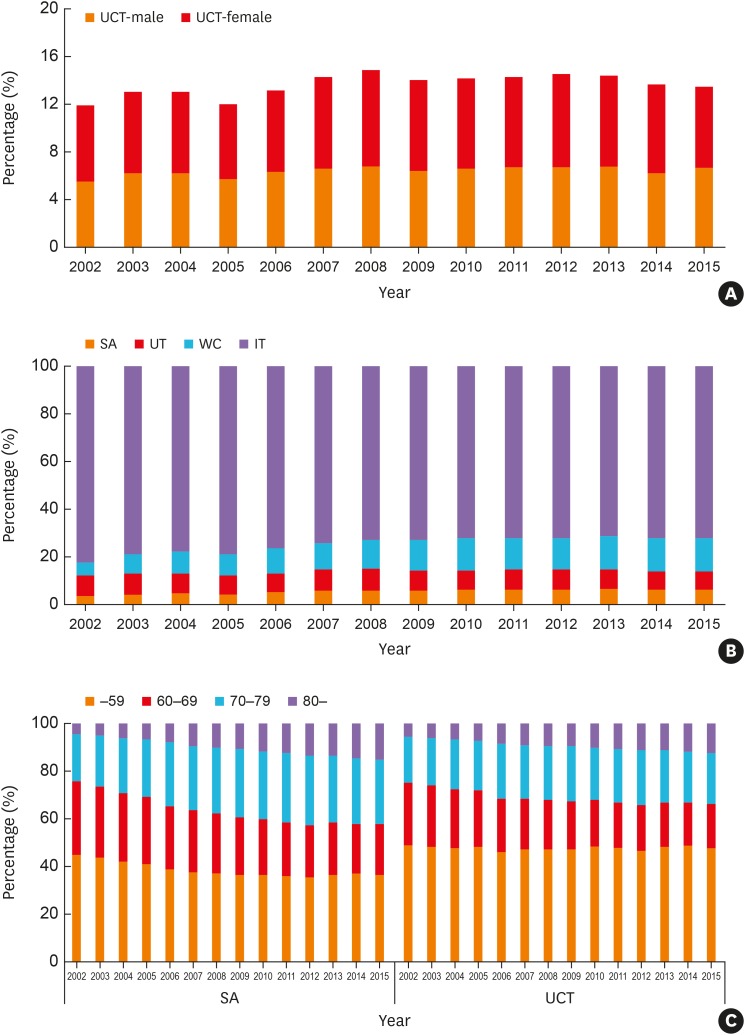
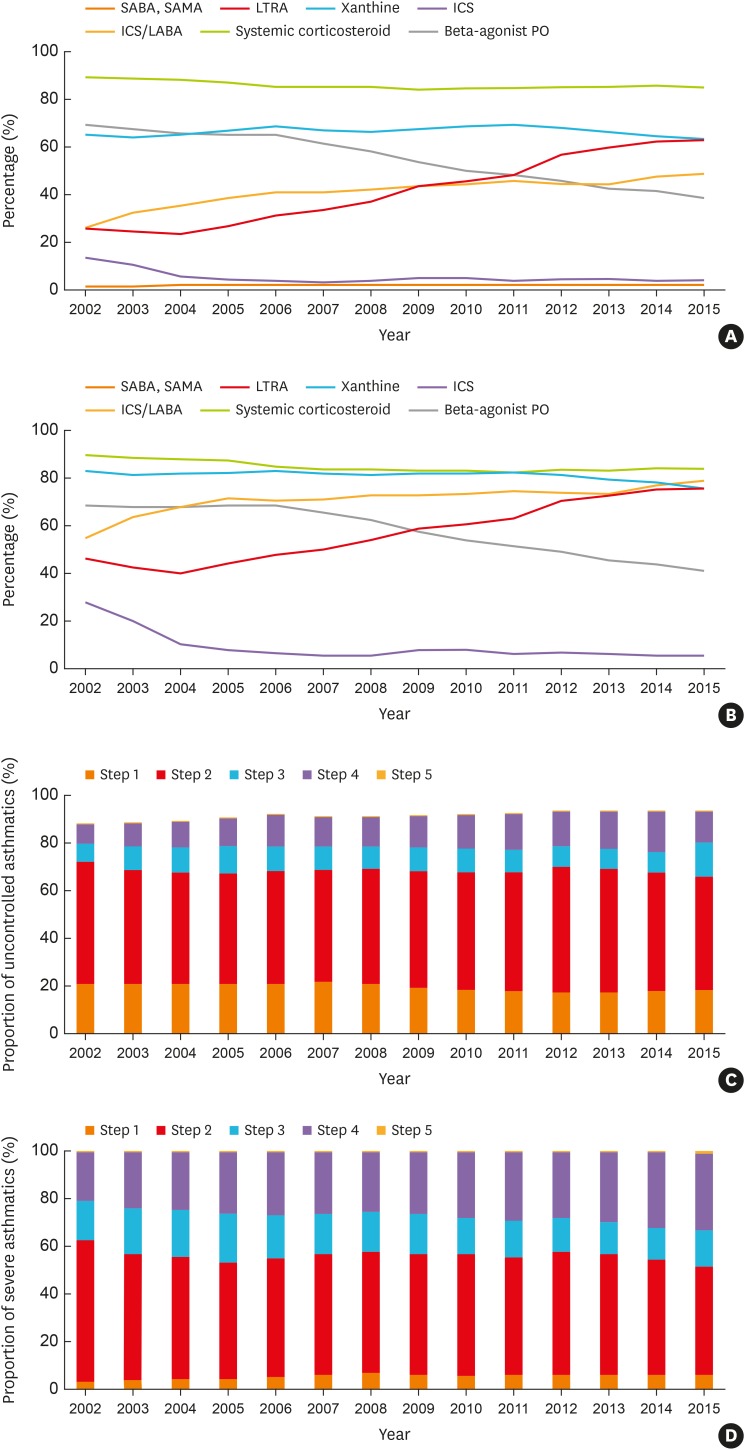
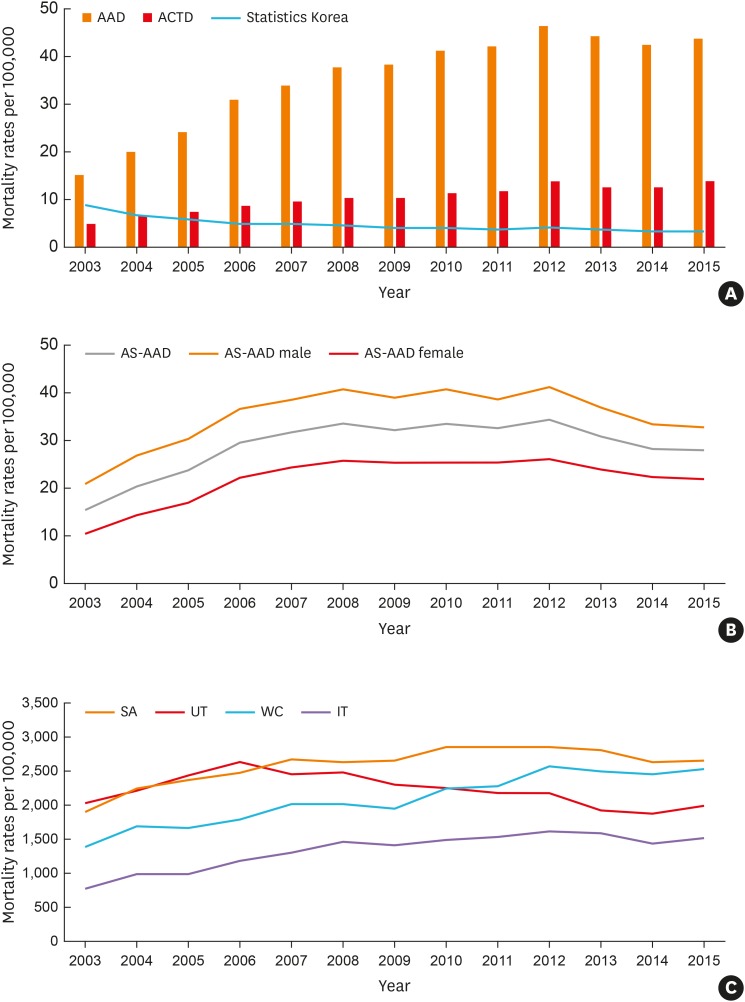
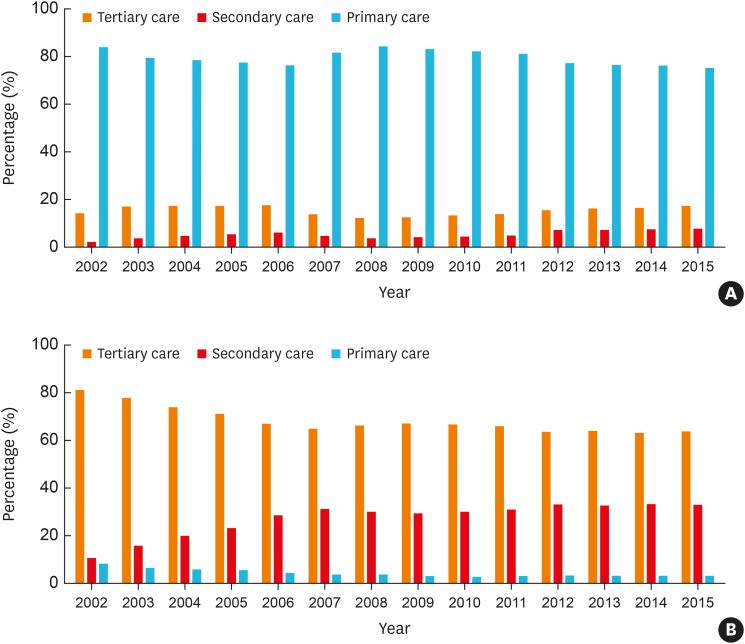
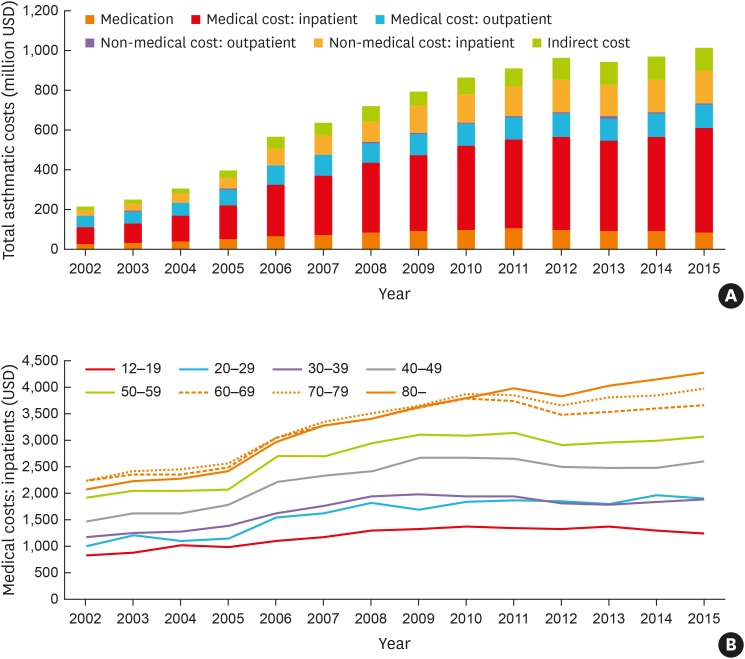
Results: The prevalence rates of asthma (1.6% to 2.2%) and severe asthma (SA; 3.5% to 6.1% among total asthmatics) have increased steadily over the decade in Korea, where the proportion of elderly asthmatics having increased. The asthma-related health care uses and costs had increased during the study period with the highest uses/costs in SA. The asthma mortality had a steady rising trend from 16.2 to 28.0 deaths per 100,000 with the highest mortality in SA.
Conclusions: The prevalence and mortality of asthma as well as SA increases along with the burden of health care uses/costs. More active interventions, including changes in health care policies, are needed to reduce the prevalence and mortality of asthma, especially SA.
Keywords: Asthma; aged; health care costs; morbidity; mortality; prevalence.
Copyright © 2020 The Korean Academy of Asthma, Allergy and Clinical Immunology · The Korean Academy of Pediatric Allergy and Respiratory Disease.
Conflict of interest statement
There are no financial or other issues that might lead to conflicts of interest.
Figures
References
-
- Crescioni M, Gorina Y, Bilheimer L, Gillum RF. Trends in Health Status and Health Care Use Among Older Men. Natl Health Stat Report. 2010:1–18. - PubMed
-
- National Health Insurance Service (KR) Status of national health insurance benefits 2004–2010 [Internet] Wonju: National Health Insurance Service; 2011. [cited 2017 Nov 22]. Available from: http://www.nhic.or.kr.
-
- Statistics Korea. Cause of death statistics [Internet] Daejeon: Korean Statistical Information Service; [cited 2017 Feb 20]. Available from: http://kosis.kr.
