

Maternal and Infant Outcomes Among Pregnant Women Treated for Multidrug/Rifampicin-Resistant Tuberculosis in South Africa
- PMID: 32141495
- PMCID: PMC8028100
- DOI: 10.1093/cid/ciaa189
Maternal and Infant Outcomes Among Pregnant Women Treated for Multidrug/Rifampicin-Resistant Tuberculosis in South Africa
Abstract
Background: Data on safety and efficacy of second-line tuberculosis drugs in pregnant women and their infants are severely limited due to exclusion from clinical trials and expanded access programs.
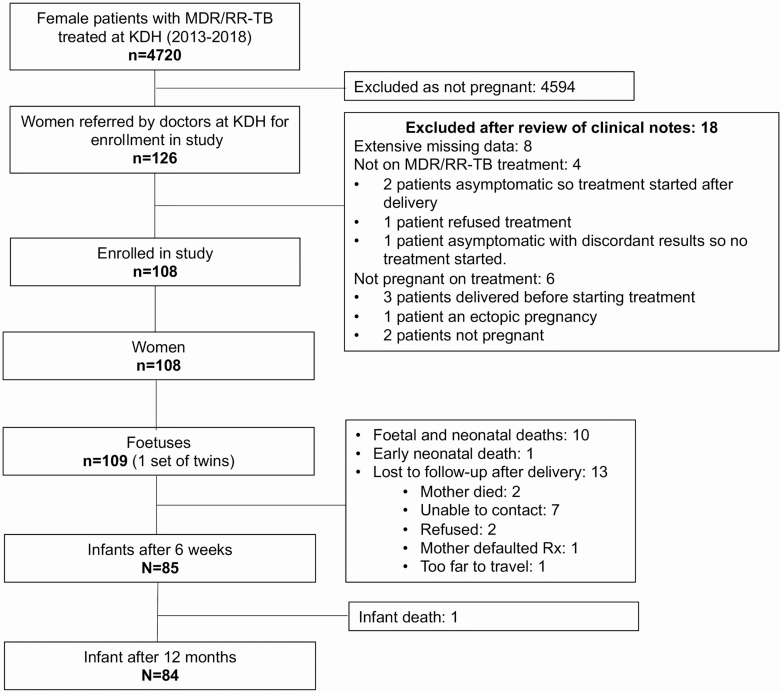
Methods: Pregnant women starting treatment for multidrug/rifampicin-resistant (MDR/RR)-tuberculosis at King Dinuzulu Hospital in KwaZulu-Natal, South Africa, from 1 January 2013 to 31 December 2017, were included. We conducted a record review to describe maternal treatment and pregnancy outcomes, and a clinical assessment to describe infant outcomes.
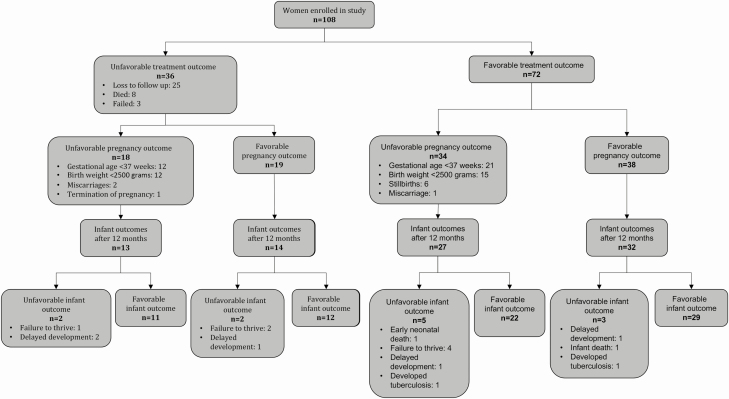
Results: Of 108 pregnant women treated for MDR/RR-tuberculosis, 88 (81%) were living with human immunodeficiency virus.. Favorable MDR/RR-tuberculosis treatment outcomes were reported in 72 (67%) women. Ninety-nine (91%) of the 109 babies were born alive, but overall, 52 (48%) women had unfavorable pregnancy outcomes. Fifty-eight (54%) women received bedaquiline, and 49 (45%) babies were exposed to bedaquiline in utero. Low birth weight was reported in more babies exposed to bedaquiline compared to babies not exposed (45% vs 26%; P = .034). In multivariate analyses, bedaquiline and levofloxacin, drugs often used in combination, were both independently associated with increased risk of low birth weight. Of the 86 children evaluated at 12 months, 72 (84%) had favorable outcomes; 88% of babies exposed to bedaquiline were thriving and developing normally compared to 82% of the babies not exposed.
Conclusions: MDR/RR-tuberculosis treatment outcomes among pregnant women were comparable to nonpregnant women. Although more babies exposed to bedaquiline were of low birth weight, over 80% had gained weight and were developing normally at 1 year.
Keywords: drug-resistant; outcome; pregnancy; treatment; tuberculosis.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Good Outcomes in Babies With In Utero Bedaquiline Exposure.Clin Infect Dis. 2021 Apr 8;72(7):1169-1170. doi: 10.1093/cid/ciaa174. Clin Infect Dis. 2021. PMID: 32141498 No abstract available.
References
-
- World Health Organization. Global tuberculosis report 2019 WHO/CDS/TB/2019.15. Geneva: World Health Organization, 2019.
-
- Mnyani CN, McIntyre JA. Tuberculosis in pregnancy. BJOG 2011; 118:226–31. - PubMed
-
- Grange J, Adhikari M, Ahmed Y, et al. . Tuberculosis in association with HIV/AIDS emerges as a major nonobstetric cause of maternal mortality in Sub-Saharan Africa. Int J Gynaecol Obstet 2010; 108:181–3. - PubMed
-
- Sugarman J, Colvin C, Moran AC, Oxlade O. Tuberculosis in pregnancy: an estimate of the global burden of disease. Lancet Glob Health 2014; 2:e710–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
