

Phase 1 study of epacadostat in combination with atezolizumab for patients with previously treated advanced nonsmall cell lung cancer
- PMID: 32141617
- PMCID: PMC7496129
- DOI: 10.1002/ijc.32951
Phase 1 study of epacadostat in combination with atezolizumab for patients with previously treated advanced nonsmall cell lung cancer
Abstract
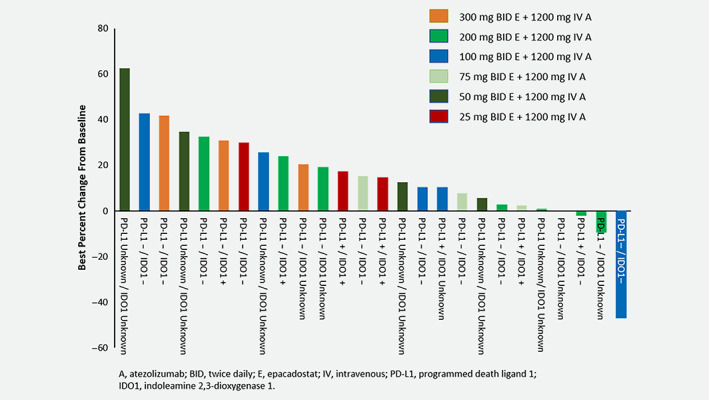
Epacadostat is a potent and highly selective inhibitor of indoleamine 2,3-dioxygenase 1 (IDO1). Here we report results from the open-label, dose-escalation, Phase 1b ECHO-110 study evaluating epacadostat plus atezolizumab in patients with previously treated Stage IIIB/IV nonsmall cell lung cancer (NSCLC). Eligible patients had received ≥1 prior line of platinum-based chemotherapy (≥2 cycles) and no prior checkpoint/IDO inhibitors treatment. Oral epacadostat (25, 50, 75, 100, 200 or 300 mg) was administered twice daily (BID) with intravenous atezolizumab 1,200 mg every 3 weeks (Q3W). Primary endpoints were safety, tolerability and dose-limiting toxicities (DLTs). Twenty-nine patients received ≥1 dose of treatment. The maximum tolerated dose of epacadostat was not reached. Two patients had DLTs: one patient with Grade 3 dehydration and hypotension (epacadostat 200 mg BID); one patient with Grade 3 hyponatremia and Grade 4 autoimmune encephalitis (epacadostat 300 mg BID). Twenty-three patients (79%) had treatment-related adverse events (AEs); seven patients (24%) experienced Grade 3/4 events; five patients (17%) discontinued treatment due to treatment-related AEs. No fatal treatment-related AEs occurred. One patient achieved a partial response (objective response rate, 3%), which was maintained for 8.3 months; eight patients had stable disease. Baseline tumoral programmed cell death ligand 1 (PD-L1) and IDO expression were low among patients with evaluable samples (1 of 23 expressed PD-L1; 5 of 17 expressed IDO). Epacadostat pharmacokinetics was comparable to historical controls. Epacadostat, at doses up to 300 mg BID, combined with atezolizumab 1,200 mg Q3W was well tolerated in patients with previously treated NSCLC, although clinical activity was limited.
Keywords: atezolizumab; combination; epacadostat; nonsmall cell lung cancer.
© 2020 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Conflict of interest statement
M.D.H. reports grants, nonfinancial support and personal fees from Bristol‐Myers Squibb; consultancy fees from Merck, Genentech/Roche, Nektar, Syndax, Mirati, Immunai and Shattuck Labs; travel support/honoraria from A7, Eli Lilly, Merck and Bristol‐Myers Squibb; consultancy fees and nonfinancial support from AstraZeneca outside the submitted work. M.D.H. also has a patent PCT/US2015/062208 licensed to PGDx. S.G. reports research funding to his institution from Bristol‐Myers Squibb, Iovance, Genentech/Roche and Takeda/Ariad; and consultancy fees from NextCure, Nektar and Bristol‐Myers Squibb. L.Q.M.C. reports minor personal consulting advisory board participation and fees from Genentech, AstraZenenca, Merck, Bristol‐Myers Squibb, Pfizer and Novartis outside the submitted work; research grant funding to her institution from Incyte and Genentech for the conduct of this study; research grant funding to her institution from Bristol‐Myers Squibb, AstraZeneca, Pfizer and Merck outside the submitted work. M.G. reports research support to his institution from Genentech. M.M.A. reports grants and personal fees from Genentech, Bristol‐Myers Squibb and AstraZeneca; personal fees from Merck, Maverick, Blueprint Medicines, Syndax, Ariad, Nektar and Gritstone and grants from Lilly outside the submitted work. E.C. reports being an employee of Genentech and owns stock in Genentech/Roche. X.G. is an employee of Incyte and owns stock in Incyte. G.Z. is an employee of Incyte and owns stock in Incyte. C.W. is an employee of Incyte and owns stock in Incyte. L.L. is an employee of Incyte and owns stock in Incyte. R.S.H. reports research support for clinical trials to her institution from Genentech/Roche, Novartis, Agios, Daichii Sankyo, Corvus, Mirati, Abbvie, Eli Lilly, Exelixis and Turning Point Therapeutics; consulting honoraria from Novartis, Boehringer Ingelheim, Tarveda, Apollomics and Chugai outside the submitted work.
Figures
References
-
- Opdivo (nivolumab) [prescribing information]. Princeton, NJ: Bristol‐Myers Squibb, 2020.
-
- Keytruda (pembrolizumab) [prescribing information]. Whitehouse Station, NJ: Merck Sharp & Dohme Corporation, 2019.
-
- Tecentriq (atezolizumab) [prescribing information]. South San Francisco, CA: Genentech, Inc., 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
