

Complexity of nursing care at 24 h from admission predicts in-hospital mortality in medical units: a cohort study
- PMID: 32143625
- PMCID: PMC7059664
- DOI: 10.1186/s12913-020-5038-5
Complexity of nursing care at 24 h from admission predicts in-hospital mortality in medical units: a cohort study
Abstract
Background: The Informative System of Nursing Performance was developed to measure complexity of nursing care based on the actual interventions performed by nurses at the point of care. The association of this score with in-hospital mortality was not investigated before. Having this information is relevant to define evidence-based criteria that hospital administrators can use to allocate nursing workforce according to the real and current patients' need for nursing care. The aim of this study is to assess the association between complexity of nursing care and in-hospital mortality.
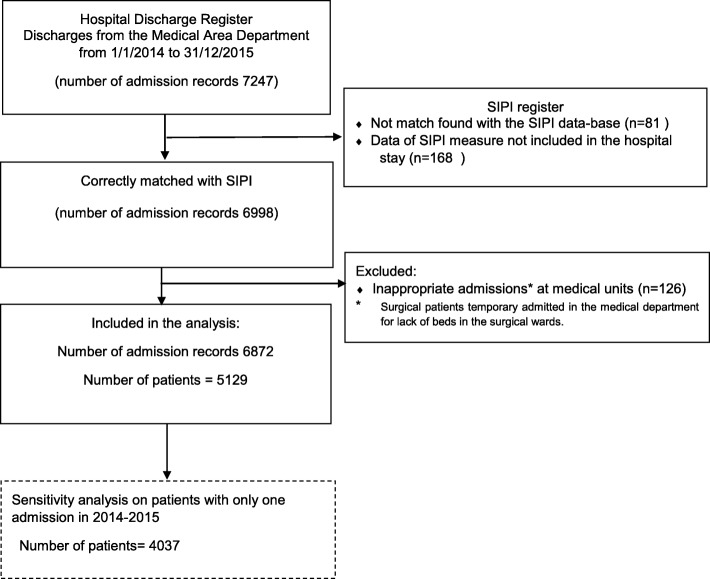
Methods: Register-based cohort study on all patients admitted to acute medical wards of a middle-large hospital in the North of Italy between January 1, 2014, to December 31, 2015 and followed up to discharge. Out of all the eligible 7247 records identified in the Hospital Discharge Register, 6872 records from 5129 patients have been included. A multivariable frailty Cox model was adopted to estimate the association between the Informative System of Nursing Performance score, both as continuous variable and dichotomized as low (score < 50) or high (score ≥ 50), and in-hospital mortality adjusting for several factors recorded at admission (age, gender, type of admission unit, type of access and Charlson Comorbidity Index).
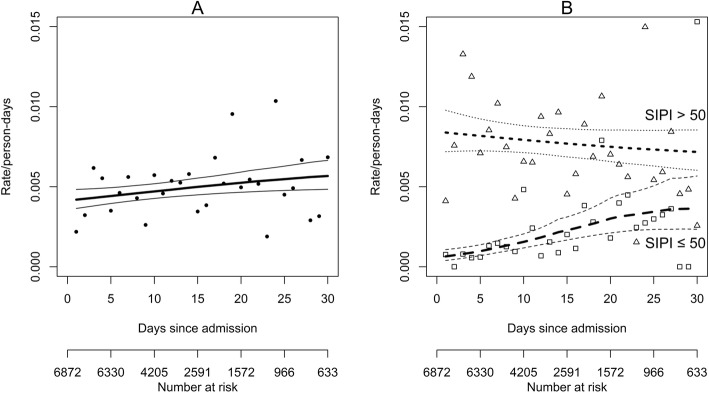
Results: The median age of the 5129 included patients was 76 [first-third quartiles 64-84] and 2657(52%) patients were males. Over the 6872 admissions, there were 395 in-hospital deaths among 2922 patients at high complexity of nursing care (13.5%) and 74/3950 (1.9%) among those at low complexity leading to a difference of 11.6% (95% CI: 10.3-13.0%). Adjusting by relevant confounders, the hazard rate of mortality in the first 10 days from admission resulted 6 times significantly higher in patients at high complexity of nursing care with respect to patients at low complexity (hazard ratio, HR 6.58, 95%CI: 4.50;9.62, p < 0.001). The HR was lower after 10 days from admission but still significantly higher than 1. By considering the continuous score, the association was confirmed.
Conclusion: Complexity of nursing care is strongly associated to in-hospital mortality of acute patients admitted to medical departments. It predicts in-hospital mortality better than widely used indicators, such as comorbidity.
Keywords: Health services research; Hospital information systems; Hospital medicine; Hospitals; Nurse staffing; Nursing care; Patient-centered care; Quality of health care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Zalkind DL, Eastaugh SR. Mortality rates as an indicator of hospital quality. Hosp Health Serv Adm. 1997;42(1):3–15. - PubMed
-
- Ben-Tovim DI, Pointer SC, Woodman R, Hakendorf PH, Harrison JE. Routine use of administrative data for safety and quality purposes--hospital mortality. Med J Aust. 2010;193(8 Suppl):S100–S103. - PubMed
-
- van Erven JA, van Galen LS, Hettinga-Roest AA, Claessens EPJ, Roos JC, Kramer MHH, et al. Hospital standardised mortality ratio: a reliable indicator of quality of care? Neth J Med. 2018;76(2):72–77. - PubMed
-
- Mitsunaga T, Hasegawa I, Uzura M, Okuno K, Otani K, Ohtaki Y, et al. Comparison of the National Early Warning Score (NEWS) and the modified early warning score (MEWS) for predicting admission and in-hospital mortality in elderly patients in the pre-hospital setting and in the emergency department. Peer J. 2019;7:e6947. doi: 10.7717/peerj.6947. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
