

A high-throughput screening platform for Polycystic Kidney Disease (PKD) drug repurposing utilizing murine and human ADPKD cells
- PMID: 32144367
- PMCID: PMC7060218
- DOI: 10.1038/s41598-020-61082-3
A high-throughput screening platform for Polycystic Kidney Disease (PKD) drug repurposing utilizing murine and human ADPKD cells
Erratum in
-
Author Correction: A high-throughput screening platform for Polycystic Kidney Disease (PKD) drug repurposing utilizing murine and human ADPKD cells.Sci Rep. 2022 Oct 13;12(1):17185. doi: 10.1038/s41598-022-21947-1. Sci Rep. 2022. PMID: 36229506 Free PMC article. No abstract available.
Abstract
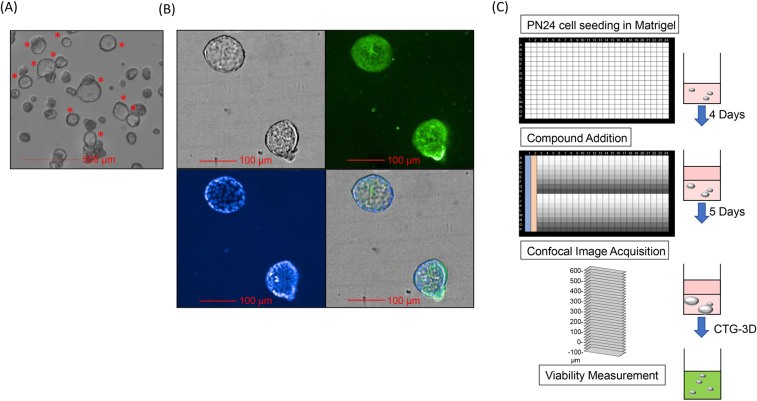
Autosomal dominant polycystic kidney disease (ADPKD) is one of the most common inherited monogenic disorders, characterized by a progressive decline in kidney function due in part to the formation of fluid-filled cysts. While there is one FDA-approved therapy, it is associated with potential adverse effects, and all other clinical interventions are largely supportive. Insights into the cellular pathways underlying ADPKD have revealed striking similarities to cancer. Moreover, several drugs originally developed for cancer have shown to ameliorate cyst formation and disease progression in animal models of ADPKD. These observations prompted us to develop a high-throughput screening platform of cancer drugs in a quest to repurpose them for ADPKD. We screened ~8,000 compounds, including compounds with oncological annotations, as well as FDA-approved drugs, and identified 155 that reduced the viability of Pkd1-null mouse kidney cells with minimal effects on wild-type cells. We found that 109 of these compounds also reduced in vitro cyst growth of Pkd1-null cells cultured in a 3D matrix. Moreover, the result of the cyst assay identified therapeutically relevant compounds, including agents that interfere with tubulin dynamics and reduced cyst growth without affecting cell viability. Because it is known that several ADPKD therapies with promising outcomes in animal models failed to be translated to human disease, our platform also incorporated the evaluation of compounds in a panel of primary ADPKD and normal human kidney (NHK) epithelial cells. Although we observed differences in compound response amongst ADPKD and NHK cell preparation, we identified 18 compounds that preferentially affected the viability of most ADPKD cells with minimal effects on NHK cells. Our study identifies attractive candidates for future efficacy studies in advanced pre-clinical models of ADPKD.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Harris, P. C. & Torres, V. E. In GeneReviews((R)) (eds Adam, M. P. et al.) (1993).
-
- Torres VE, Rossetti S, Harris PC. Update on autosomal dominant polycystic kidney disease. Minerva Med. 2007;98:669–691. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
