

Diagnostic test accuracy of ADC values for identification of clear cell renal cell carcinoma: systematic review and meta-analysis
- PMID: 32144458
- PMCID: PMC7315585
- DOI: 10.1007/s00330-020-06740-w
Diagnostic test accuracy of ADC values for identification of clear cell renal cell carcinoma: systematic review and meta-analysis
Abstract
Objectives: To perform a systematic review on apparent diffusion coefficient (ADC) values of renal tumor subtypes and meta-analysis on the diagnostic performance of ADC for differentiation of localized clear cell renal cell carcinoma (ccRCC) from other renal tumor types.
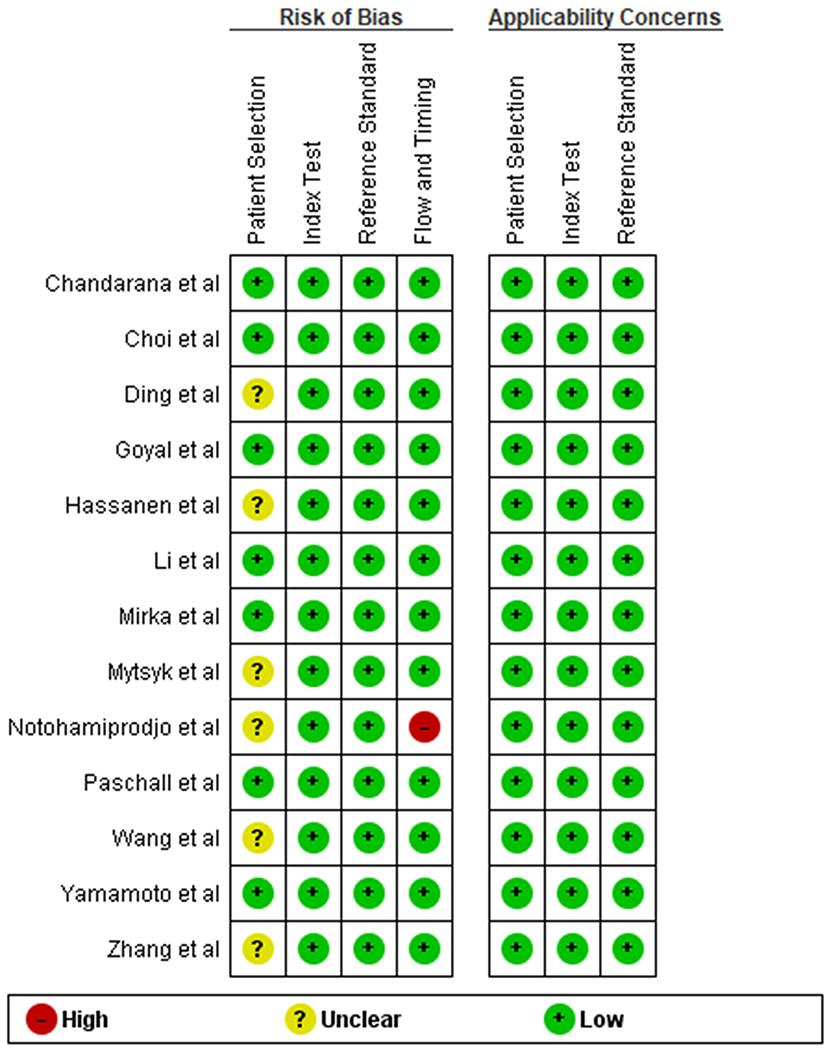
Methods: Medline, Embase, and the Cochrane Library databases were searched for studies published until May 1, 2019, that reported ADC values of renal tumors. Methodological quality was evaluated. For the meta-analysis on diagnostic test accuracy of ADC for differentiation of ccRCC from other renal lesions, we applied a bivariate random-effects model and compared two subgroups of ADC measurement with vs. without cystic and necrotic areas.
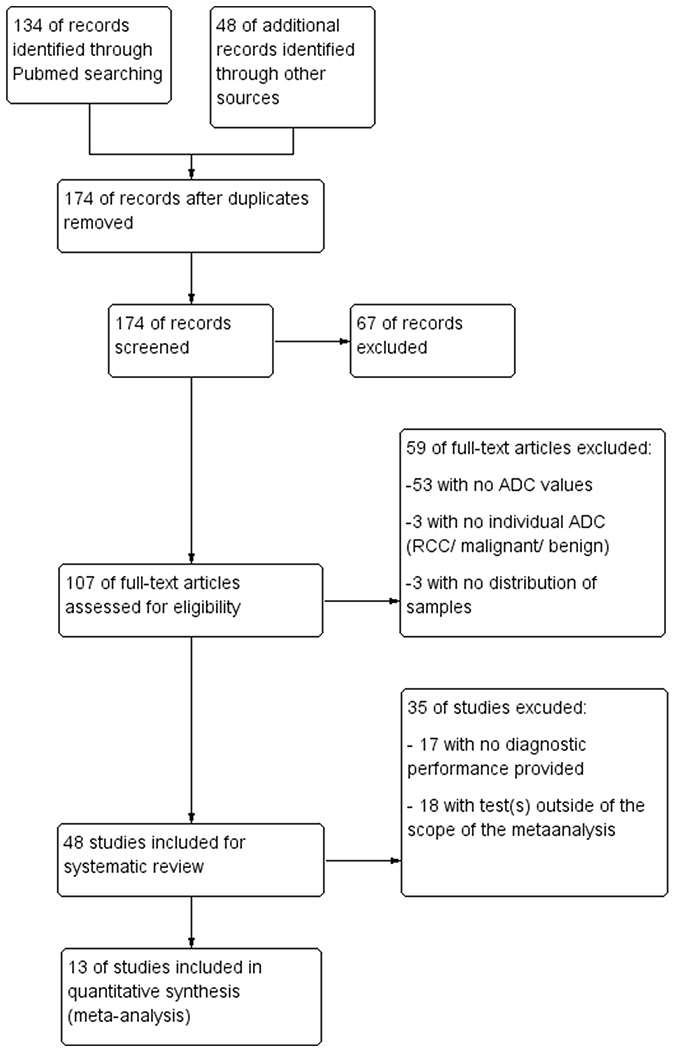
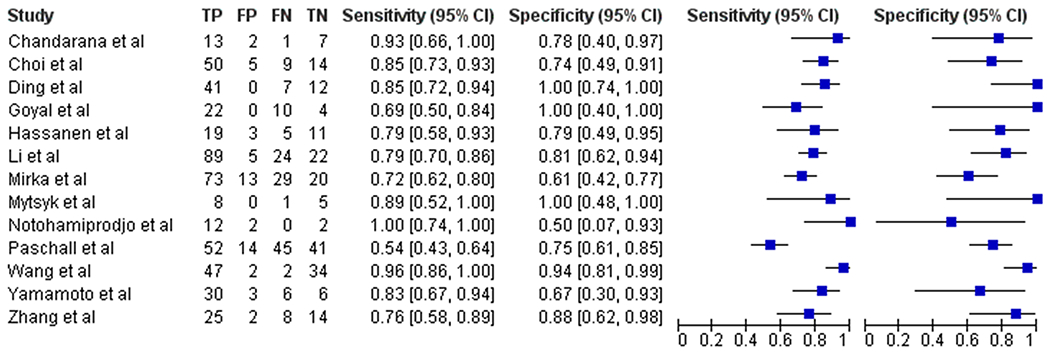
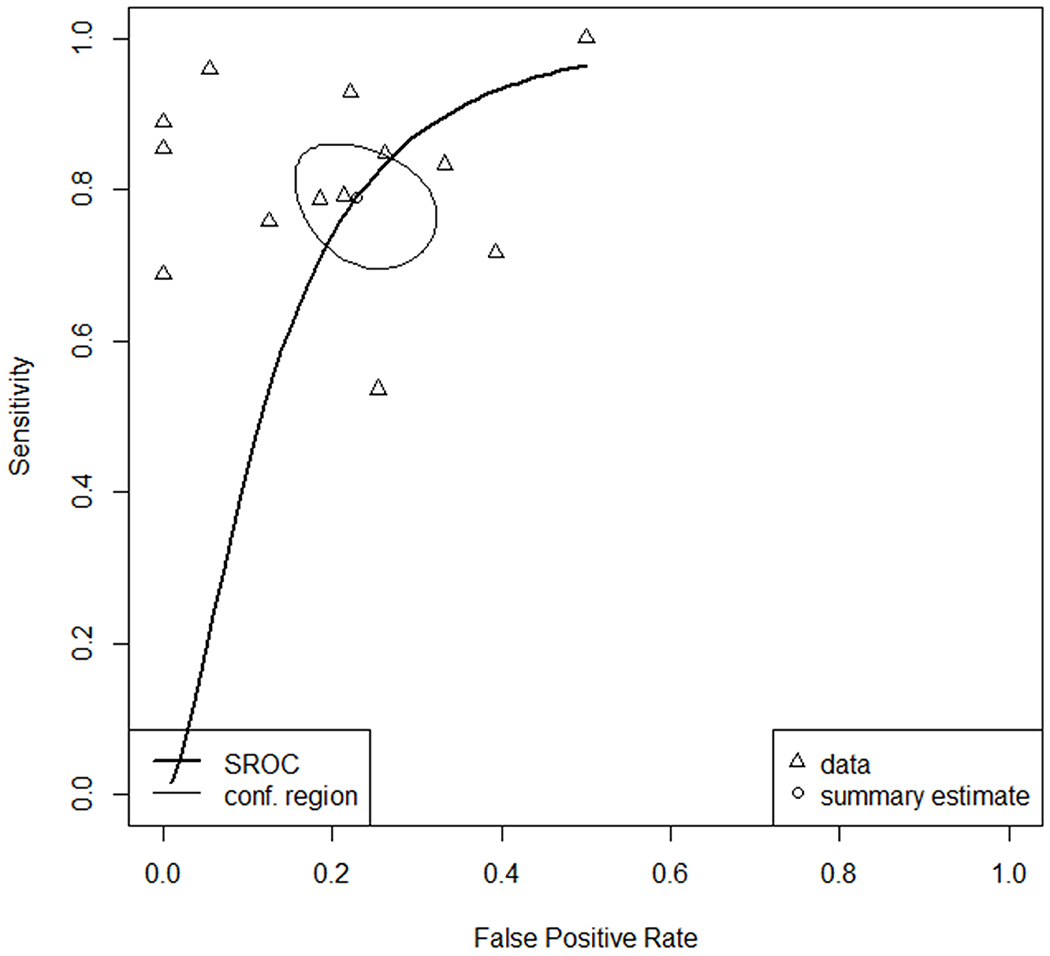
Results: We included 48 studies (2588 lesions) in the systematic review and 13 studies (1126 lesions) in the meta-analysis. There was no significant difference in ADC of renal parenchyma using b values of 0-800 vs. 0-1000 (p = 0.08). ADC measured on selected portions (sADC) excluding cystic and necrotic areas differed significantly from whole-lesion ADC (wADC) (p = 0.002). Compared to ccRCC, minimal-fat angiomyolipoma, papillary RCC, and chromophobe RCC showed significantly lower sADC while oncocytoma exhibited higher sADC. Summary estimates of sensitivity and specificity to differentiate ccRCC from other tumors were 80% (95% CI, 0.76-0.88) and 78% (95% CI, 0.64-0.89), respectively, for sADC and 77% (95% CI, 0.59-0.90) and 77% (95% CI, 0.69-0.86) for wADC. sADC offered a higher area under the receiver operating characteristic curve than wADC (0.852 vs. 0.785, p = 0.02).
Conclusions: ADC values of kidney tumors that exclude cystic or necrotic areas more accurately differentiate ccRCC from other renal tumor types than whole-lesion ADC values.
Key points: • Selective ADC of renal tumors, excluding cystic and necrotic areas, provides better discriminatory ability than whole-lesion ADC to differentiate clear cell RCC from other renal lesions, with area under the receiver operating characteristic curve (AUC) of 0.852 vs. 0.785, respectively (p = 0.02). • Selective ADC of renal masses provides moderate sensitivity and specificity of 80% and 78%, respectively, for differentiation of clear cell renal cell carcinoma (RCC) from papillary RCC, chromophobe RCC, oncocytoma, and minimal-fat angiomyolipoma. • Selective ADC excluding cystic and necrotic areas are preferable to whole-lesion ADC as an additional tool to multiphasic MRI to differentiate clear cell RCC from other renal lesions whether the highest b value is 800 or 1000.
Keywords: Clear cell renal cell carcinoma; Diffusion weighted imaging; Kidney neoplasms; Renal cell carcinoma.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
