

Ending the HIV epidemic in the USA: an economic modelling study in six cities
- PMID: 32145760
- PMCID: PMC7338235
- DOI: 10.1016/S2352-3018(20)30033-3
Ending the HIV epidemic in the USA: an economic modelling study in six cities
Abstract
Background: The HIV epidemic in the USA is a collection of diverse local microepidemics. We aimed to identify optimal combination implementation strategies of evidence-based interventions to reach 90% reduction of incidence in 10 years, in six US cities that comprise 24·1% of people living with HIV in the USA.
Methods: In this economic modelling study, we used a dynamic HIV transmission model calibrated with the best available evidence on epidemiological and structural conditions for six US cities: Atlanta (GA), Baltimore (MD), Los Angeles (CA), Miami (FL), New York City (NY), and Seattle (WA). We assessed 23 040 combinations of 16 evidence-based interventions (ie, HIV prevention, testing, treatment, engagement, and re-engagement) to identify combination strategies providing the greatest health benefit while remaining cost-effective. Main outcomes included averted HIV infections, quality-adjusted life-years (QALYs), total cost (in 2018 US$), and incremental cost-effectiveness ratio (ICER; from the health-care sector perspective, 3% annual discount rate). Interventions were implemented at previously documented and ideal (90% coverage or adoption) scale-up, and sustained from 2020 to 2030, with outcomes evaluated until 2040.
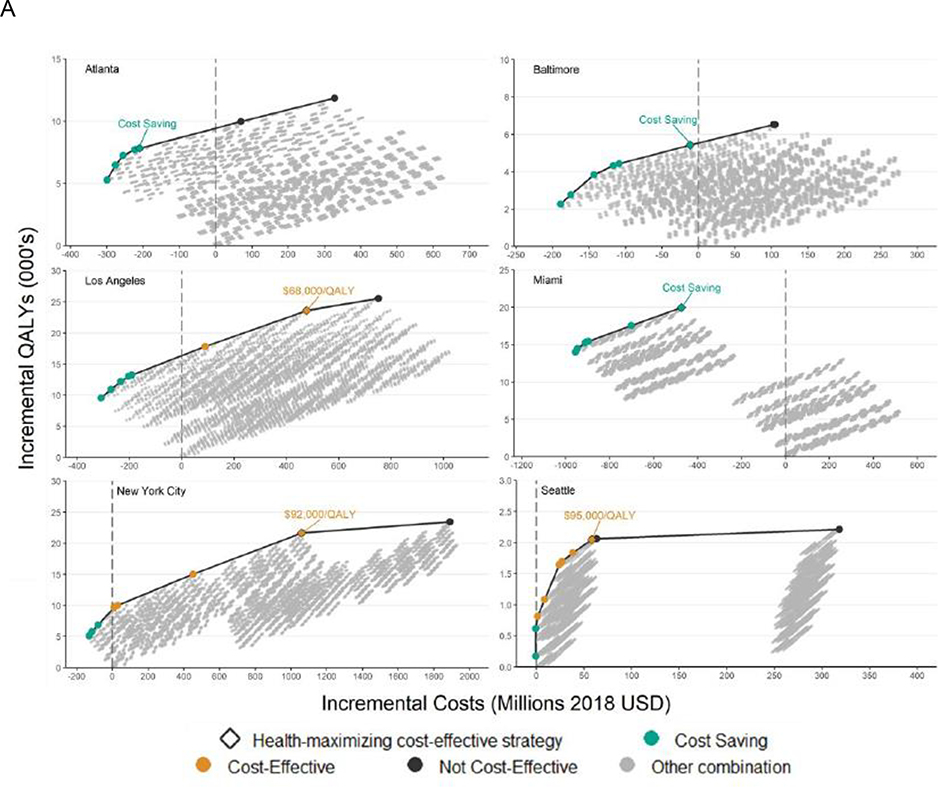
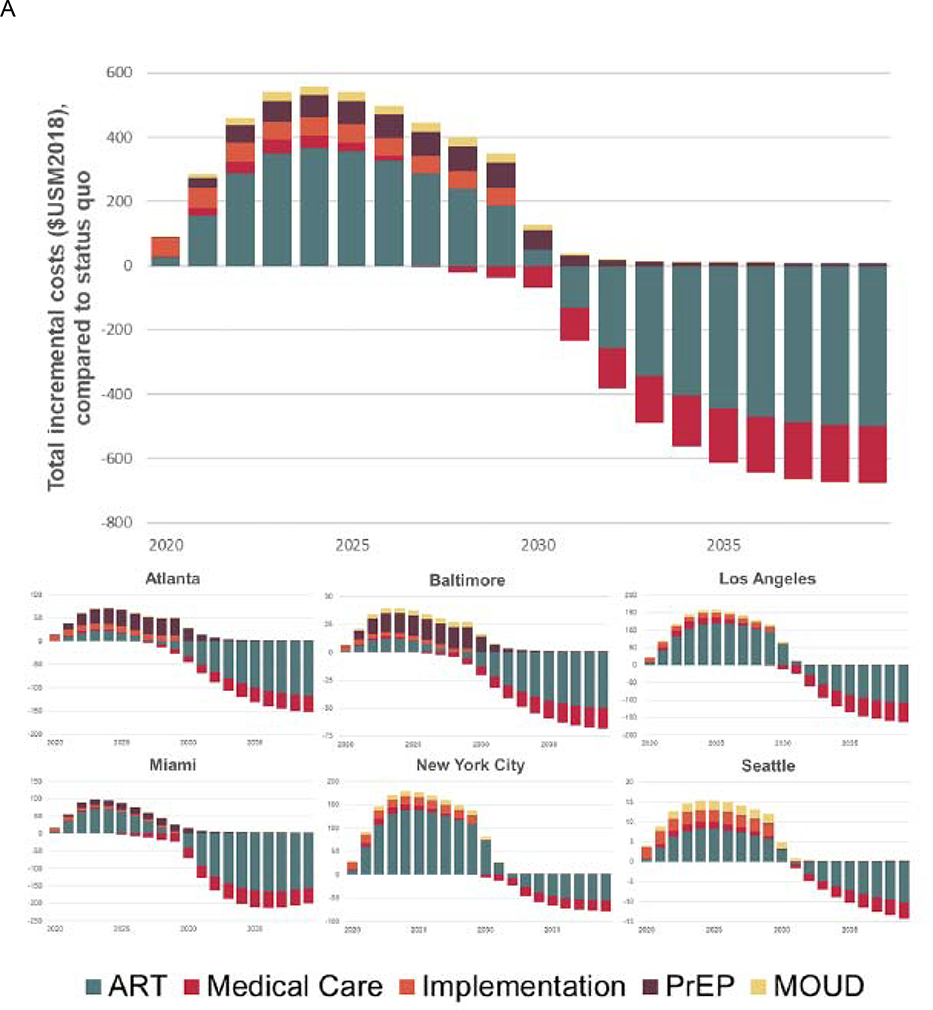
Findings: Optimal combination strategies providing health benefit and cost-effectiveness contained between nine (Seattle) and 13 (Miami) individual interventions. If implemented at previously documented scale-up, these strategies could reduce incidence by between 30·7% (95% credible interval 19·1-43·7; Seattle) and 50·1% (41·5-58·0; New York City) by 2030, at ICERs ranging from cost-saving in Atlanta, Baltimore, and Miami, to $95 416 per QALY in Seattle. Incidence reductions reached between 39·5% (26·3-53·8) in Seattle and 83·6% (70·8-87·0) in Baltimore at ideal implementation. Total costs of implementing strategies across the cities at previously documented scale-up reached $559 million per year in 2024; however, costs were offset by long-term reductions in new infections and delayed disease progression, with Atlanta, Baltimore, and Miami projecting cost savings over the 20 year study period.
Interpretation: Evidence-based interventions can deliver substantial public health and economic value; however, complementary strategies to overcome social and structural barriers to HIV care will be required to reach national targets of the ending the HIV epidemic initiative by 2030.
Funding: National Institutes of Health.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures



Comment in
-
Ending the HIV epidemic in the USA.Lancet HIV. 2020 Jul;7(7):e454-e455. doi: 10.1016/S2352-3018(20)30051-5. Epub 2020 Mar 5. Lancet HIV. 2020. PMID: 32145761 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC). HIV surveillance--United States, 1981–2008. MMWR Morbidity and mortality weekly report 2011; 60(21): 689. - PubMed
-
- Centers for Disease Control and Prevention (CDC). HIV Surveillance Report, 2017; vol. 29 Atlanta, GA: U.S. Department of Health and Human Services, 2018.
-
- Fauci AS, Redfield RR, Sigounas G, Weahkee MD, Giroir BP. Ending the HIV epidemic: a plan for the United States. Journal of the American Medical Association 2019; 321(9): 844–5. - PubMed
