

Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): a phase 3, open-label, randomised controlled trial
- PMID: 32145825
- PMCID: PMC7181180
- DOI: 10.1016/S0140-6736(20)30415-3
Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): a phase 3, open-label, randomised controlled trial
Abstract
Background: Urothelial carcinomas of the upper urinary tract (UTUCs) are rare, with poorer stage-for-stage prognosis than urothelial carcinomas of the urinary bladder. No international consensus exists on the benefit of adjuvant chemotherapy for patients with UTUCs after nephroureterectomy with curative intent. The POUT (Peri-Operative chemotherapy versus sUrveillance in upper Tract urothelial cancer) trial aimed to assess the efficacy of systemic platinum-based chemotherapy in patients with UTUCs.
Methods: We did a phase 3, open-label, randomised controlled trial at 71 hospitals in the UK. We recruited patients with UTUC after nephroureterectomy staged as either pT2-T4 pN0-N3 M0 or pTany N1-3 M0. We randomly allocated participants centrally (1:1) to either surveillance or four 21-day cycles of chemotherapy, using a minimisation algorithm with a random element. Chemotherapy was either cisplatin (70 mg/m2) or carboplatin (area under the curve [AUC]4·5/AUC5, for glomerular filtration rate <50 mL/min only) administered intravenously on day 1 and gemcitabine (1000 mg/m2) administered intravenously on days 1 and 8; chemotherapy was initiated within 90 days of surgery. Follow-up included standard cystoscopic, radiological, and clinical assessments. The primary endpoint was disease-free survival analysed by intention to treat with a Peto-Haybittle stopping rule for (in)efficacy. The trial is registered with ClinicalTrials.gov, NCT01993979. A preplanned interim analysis met the efficacy criterion for early closure after recruitment of 261 participants.
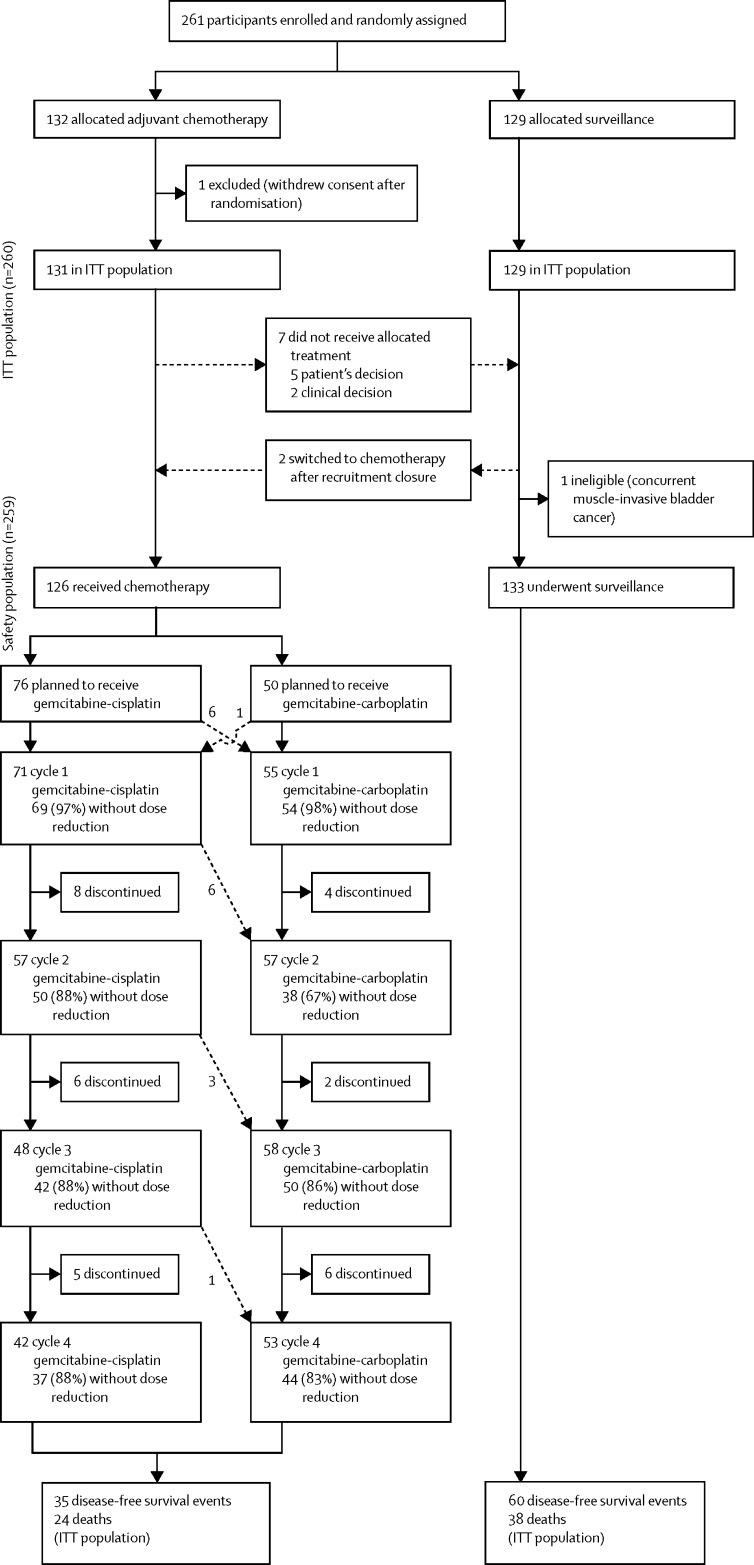
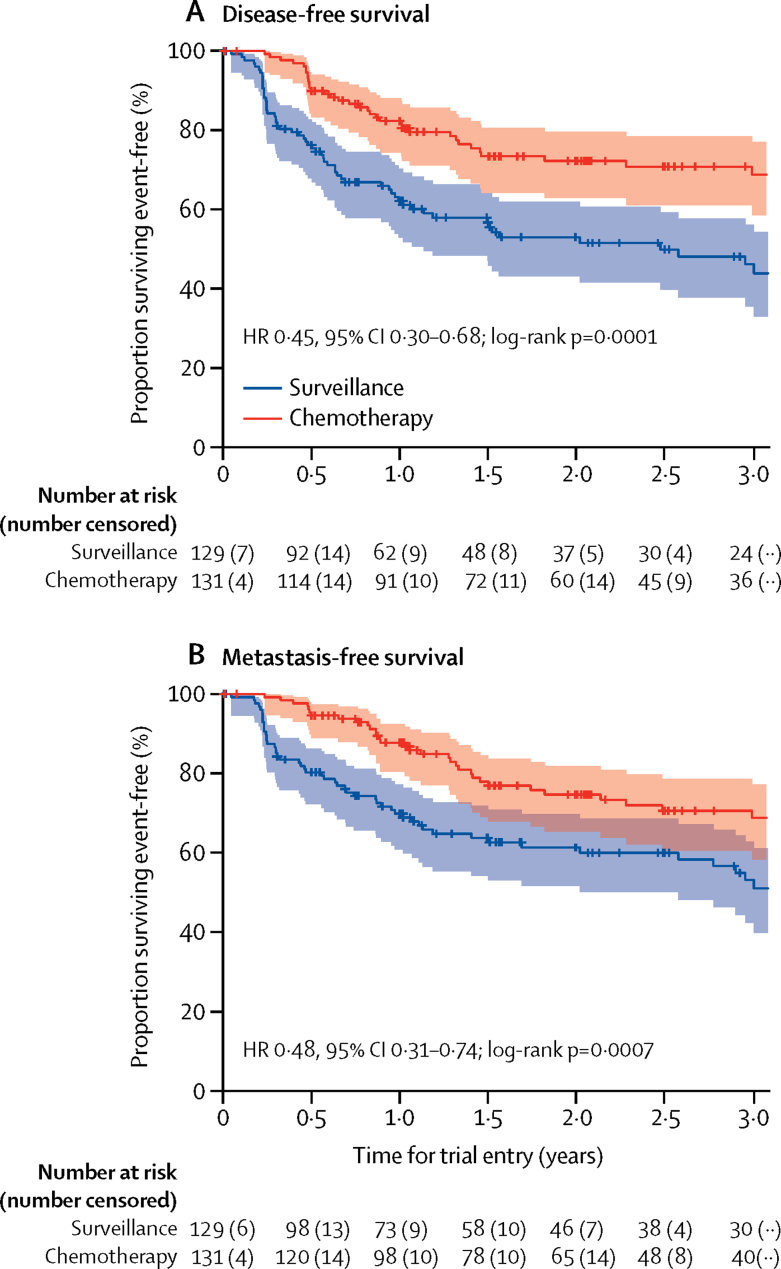
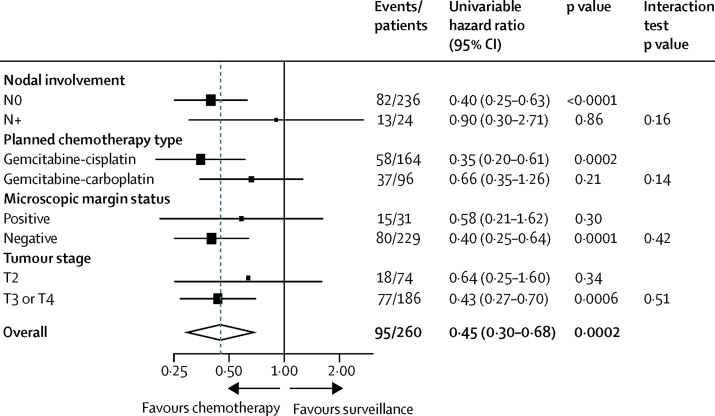
Findings: Between June 19, 2012, and Nov 8, 2017, we enrolled 261 participants from 57 of 71 open study sites. 132 patients were assigned chemotherapy and 129 surveillance. One participant allocated chemotherapy withdrew consent for data use after randomisation and was excluded from analyses. Adjuvant chemotherapy significantly improved disease-free survival (hazard ratio 0·45, 95% CI 0·30-0·68; p=0·0001) at a median follow-up of 30·3 months (IQR 18·0-47·5). 3-year event-free estimates were 71% (95% CI 61-78) and 46% (36-56) for chemotherapy and surveillance, respectively. 55 (44%) of 126 participants who started chemotherapy had acute grade 3 or worse treatment-emergent adverse events, which accorded with frequently reported events for the chemotherapy regimen. Five (4%) of 129 patients managed by surveillance had acute grade 3 or worse emergent adverse events. No treatment-related deaths were reported.
Interpretation: Gemcitabine-platinum combination chemotherapy initiated within 90 days after nephroureterectomy significantly improved disease-free survival in patients with locally advanced UTUC. Adjuvant platinum-based chemotherapy should be considered a new standard of care after nephroureterectomy for this patient population.
Funding: Cancer Research UK.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Treatment of upper urinary tract urothelial carcinoma.Lancet. 2020 Apr 18;395(10232):1232-1234. doi: 10.1016/S0140-6736(20)30519-5. Epub 2020 Mar 5. Lancet. 2020. PMID: 32145828 No abstract available.
-
New standard for localized UTUC.Nat Rev Clin Oncol. 2020 May;17(5):275. doi: 10.1038/s41571-020-0354-6. Nat Rev Clin Oncol. 2020. PMID: 32203273 No abstract available.
-
New standard for localized UTUC.Nat Rev Urol. 2020 Jul;17(7):370. doi: 10.1038/s41585-020-0308-x. Nat Rev Urol. 2020. PMID: 32203309 No abstract available.
-
Re: Adjuvant Chemotherapy in Upper Tract Urothelial Carcinoma (the POUT Trial): A Phase 3, Open-label, Randomised Controlled Trial.Eur Urol. 2020 Aug;78(2):289-290. doi: 10.1016/j.eururo.2020.04.006. Epub 2020 Apr 28. Eur Urol. 2020. PMID: 32359702 No abstract available.
-
Re: Adjuvant Chemotherapy in Upper Tract Urothelial Carcinoma (the POUT Trial): A Phase 3, Open-label, Randomised Controlled Trial.Eur Urol. 2020 Oct;78(4):630-631. doi: 10.1016/j.eururo.2020.04.021. Epub 2020 May 22. Eur Urol. 2020. PMID: 32451179 No abstract available.
-
[Adjuvant chemotherapy in the treatment of urothelial carcinoma of the upper urinary tract].Strahlenther Onkol. 2020 Sep;196(9):837-840. doi: 10.1007/s00066-020-01640-w. Strahlenther Onkol. 2020. PMID: 32561938 German. No abstract available.
-
Re: Adjuvant Chemotherapy in Upper Tract Urothelial Carcinoma (the POUT Trial): A Phase 3, Open-label, Randomised Controlled Trial.Eur Urol. 2021 Jan;79(1):163-164. doi: 10.1016/j.eururo.2020.08.015. Epub 2020 Sep 24. Eur Urol. 2021. PMID: 32981804 No abstract available.
-
Re: Alison Birtle, Mark Johnson, John Chester, et al. Adjuvant Chemotherapy in Upper Tract Urothelial Carcinoma (the POUT Trial): A Phase 3, Open-label, Randomised Controlled Trial. Lancet 2020;395:1268-77: A New Standard for a Rare Disease? Optimizing the Timing of Chemotherapy for Upper Tract Urothelial Carcinoma.Eur Urol. 2021 Jan;79(1):e28. doi: 10.1016/j.eururo.2020.09.013. Epub 2020 Sep 30. Eur Urol. 2021. PMID: 33008662 No abstract available.
References
-
- Roupret M, Babjuk M, Comperat E. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2017 update. Eur Urol. 2018;73:111–122. - PubMed
-
- Audenet F, Yates DR, Cussenot O, Rouprêt M. The role of chemotherapy in the treatment of urothelial cell carcinoma of the upper urinary tract (UUT-UCC) Urol Oncol. 2013;31:407–413. - PubMed
-
- Loehrer PJ, Sr, Einhorn LH, Elson PJ. A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: a cooperative group study. J Clin Oncol. 1992;10:1066–1073. - PubMed
-
- Sternberg CN, Skoneczna I, Kerst JM. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): an intergroup, open-label, randomised phase 3 trial. Lancet Oncol. 2015;16:76–86. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
