

Sepsis trends: increasing incidence and decreasing mortality, or changing denominator?
- PMID: 32148931
- PMCID: PMC7024753
- DOI: 10.21037/jtd.2019.12.51
Sepsis trends: increasing incidence and decreasing mortality, or changing denominator?
Abstract
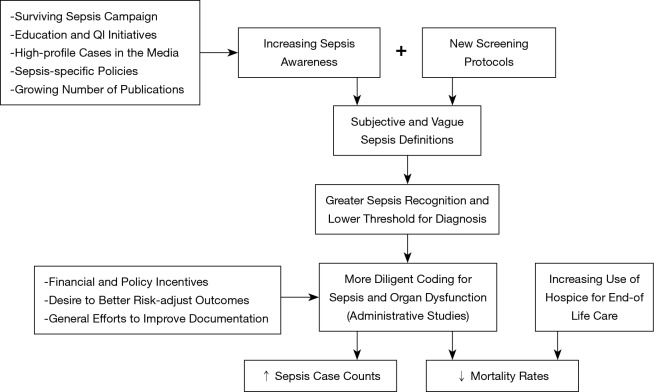
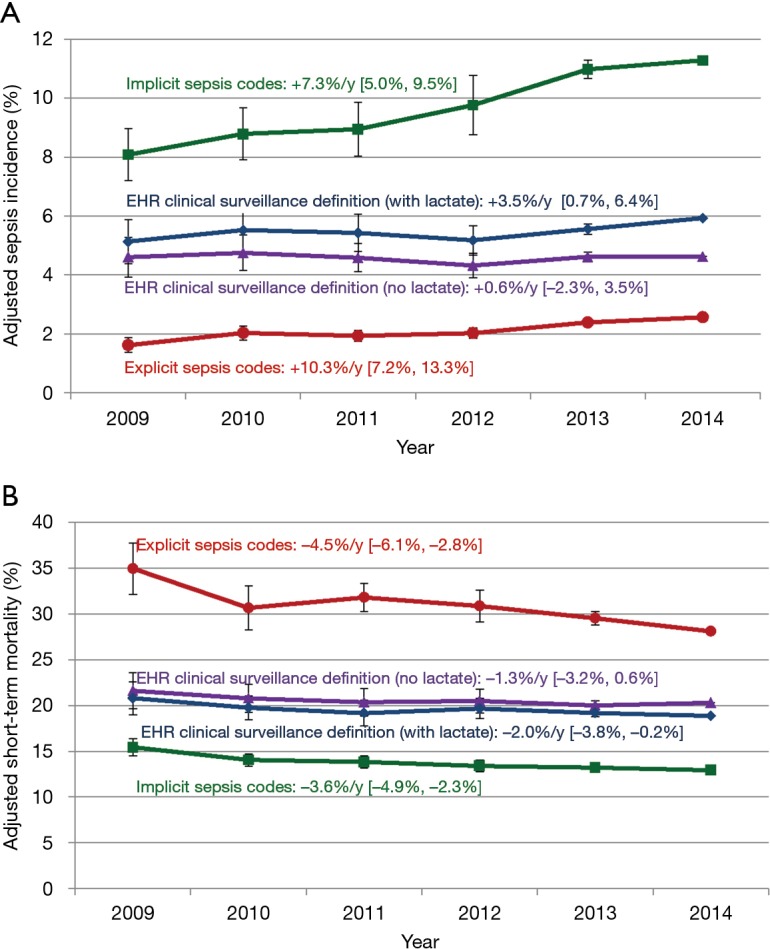
Numerous studies suggest that the incidence of sepsis has been steadily increasing over the past several decades while mortality rates are falling. However, reliably assessing trends in sepsis epidemiology is challenging due to changing diagnosis and coding practices over time. Ongoing efforts by clinicians, administrators, policy makers, and patient advocates to increase sepsis awareness, screening, and recognition are leading to more patients being labeled with sepsis. Subjective clinical definitions and heterogeneous presentations also allow for wide discretion in diagnosing sepsis rather than specific infections alone or non-specific syndromes. These factors create a potential ascertainment bias whereby the inclusion of less severely ill patients in sepsis case counts over time leads to a perceived increase in sepsis incidence and decrease in sepsis mortality rates. Analyses that rely on administrative data alone are further confounded by changing coding practices in response to new policies, financial incentives, and efforts to improve documentation. An alternate strategy for measuring sepsis incidence, outcomes, and trends is to use objective and consistent clinical criteria rather than administrative codes or registries to identify sepsis. This is feasible using data routinely found in electronic health record systems, such as blood culture draws and sustained courses of antibiotics to identify infection and laboratory values, vasopressors, and mechanical ventilation to measure acute organ dysfunction. Recent surveillance studies using this approach suggest that sepsis incidence and mortality rates have been essentially stable over the past decade. In this review, we summarize the major epidemiologic studies of sepsis trends, potential biases in these analyses, and the recent change in the surveillance paradigm toward using objective clinical data from electronic health records to more accurately characterize sepsis trends.
Keywords: Sepsis; incidence; surveillance; trends.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Rubens M, Saxena A, Ramamoorthy V, et al. Increasing Sepsis Rates in the United States: Results From National Inpatient Sample, 2005 to 2014. J Intensive Care Med 2018:885066618794136. [Epub ahead of print]. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous