

Time to stop randomized and large pragmatic trials for intensive care medicine syndromes: the case of sepsis and acute respiratory distress syndrome
- PMID: 32148932
- PMCID: PMC7024757
- DOI: 10.21037/jtd.2019.10.36
Time to stop randomized and large pragmatic trials for intensive care medicine syndromes: the case of sepsis and acute respiratory distress syndrome
Abstract
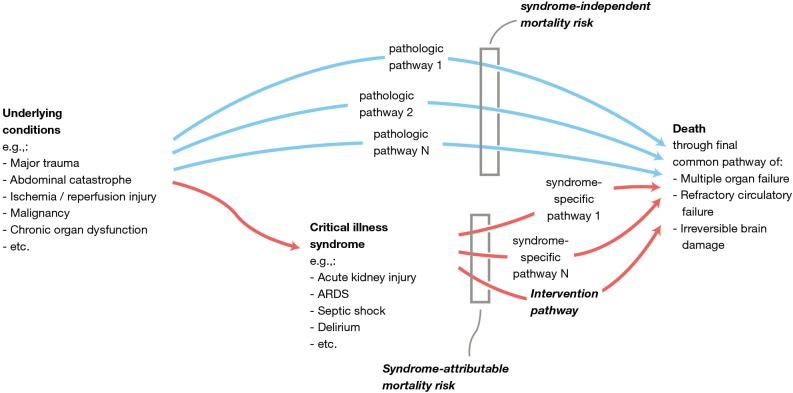
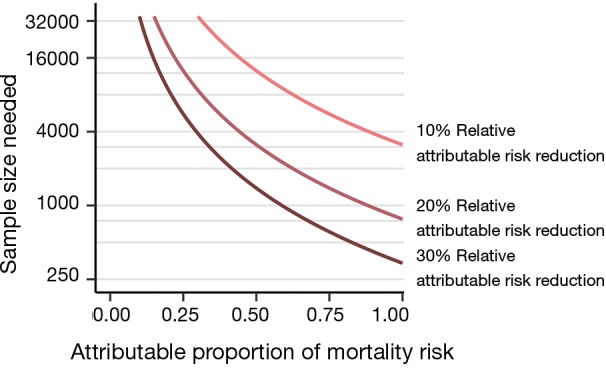
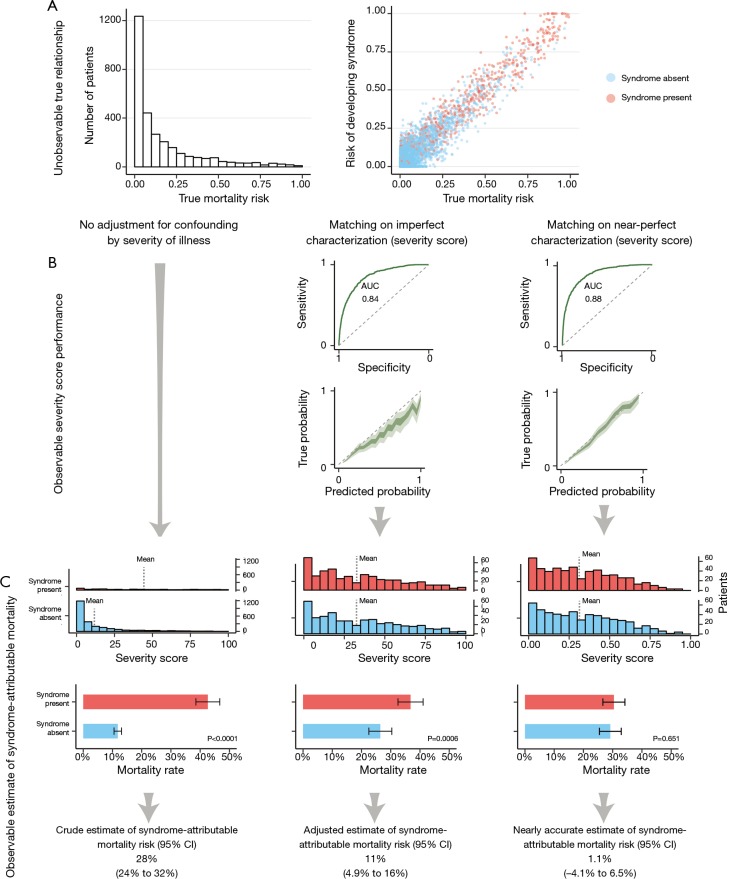
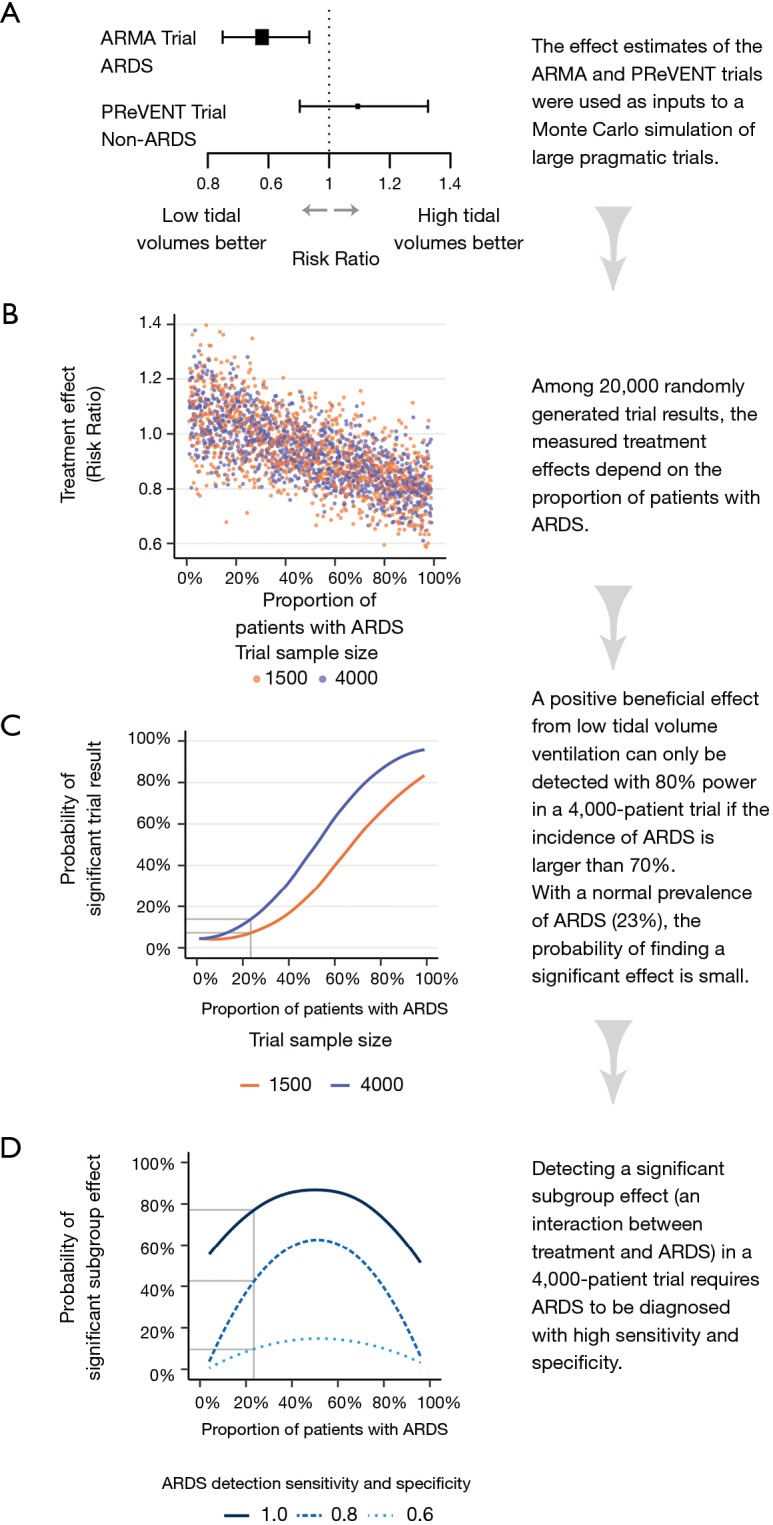
In this paper we discuss the limitations of large randomized controlled trials with mortality endpoints in patients with critical illness associated diagnoses such as sepsis. When patients with the same syndrome diagnosis do not share the pathways that lead to death (the attributable risk), any therapy can only lead to small effects in these populations. Using Monte Carlo simulations, we show how the syndrome-attributable risks of critical illness-associated diagnoses are likely overestimated using common statistical methods. This overestimation of syndrome-attributable risks leads to a corresponding overestimation of attainable treatment effects and an underestimation of required sample sizes. We demonstrate that larger and more 'pragmatic' randomized trials are not the solution because they decrease therapeutic and diagnostic precision, the therapeutic effect size and the probability of finding a beneficial effect. Finally, we argue that the most logical solution is a renewed focus on mechanistic research into the complexities of critical illness syndromes.
Keywords: Acute respiratory distress syndrome (ARDS); Monte Carlo simulation; clinical trials; research methods.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Medical