

Preoperative Portal Vein Embolization in Hepatic Surgery: A Review about the Embolic Materials and Their Effects on Liver Regeneration and Outcome
- PMID: 32148959
- PMCID: PMC7054797
- DOI: 10.1155/2020/9295852
Preoperative Portal Vein Embolization in Hepatic Surgery: A Review about the Embolic Materials and Their Effects on Liver Regeneration and Outcome
Abstract
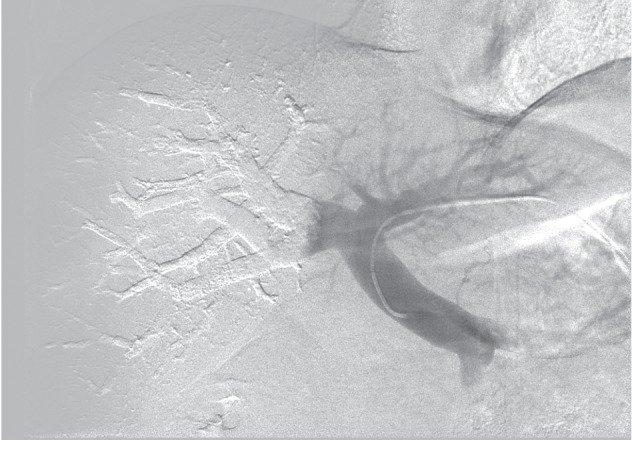
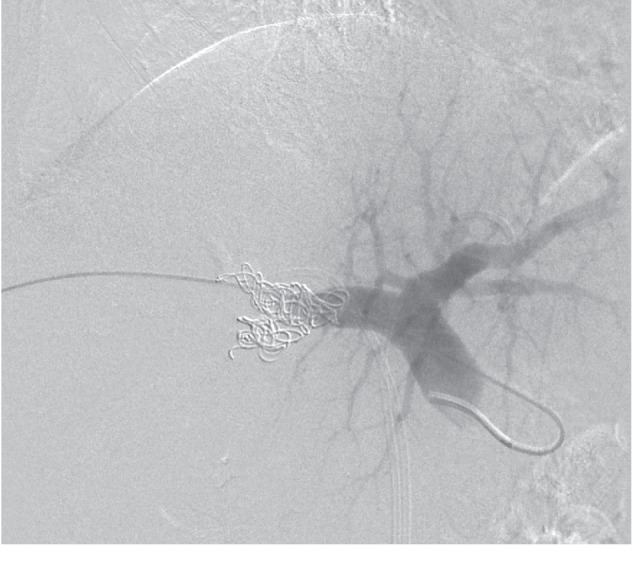
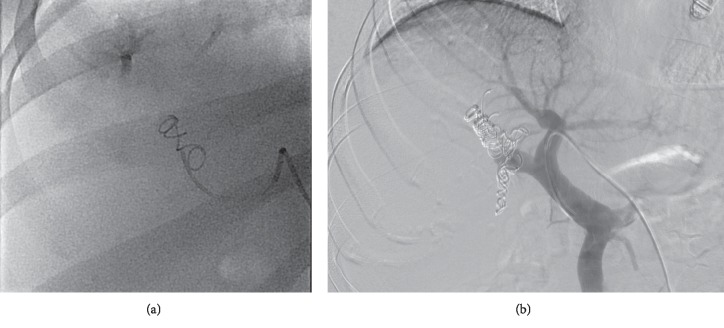
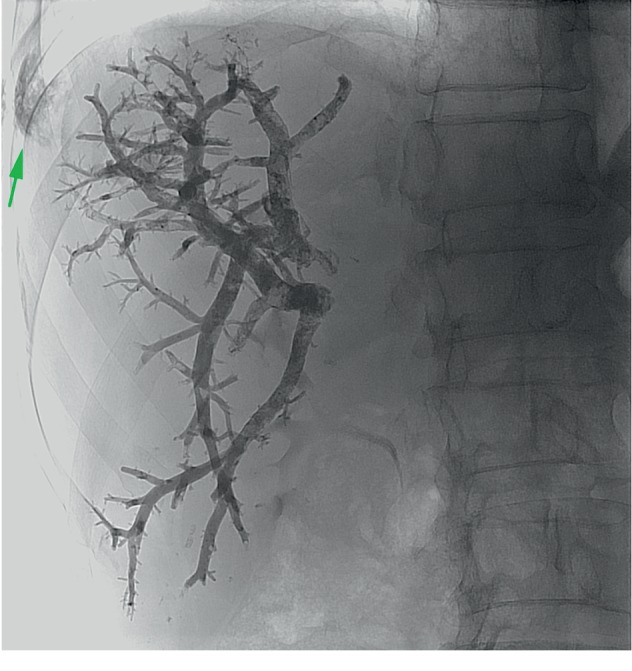
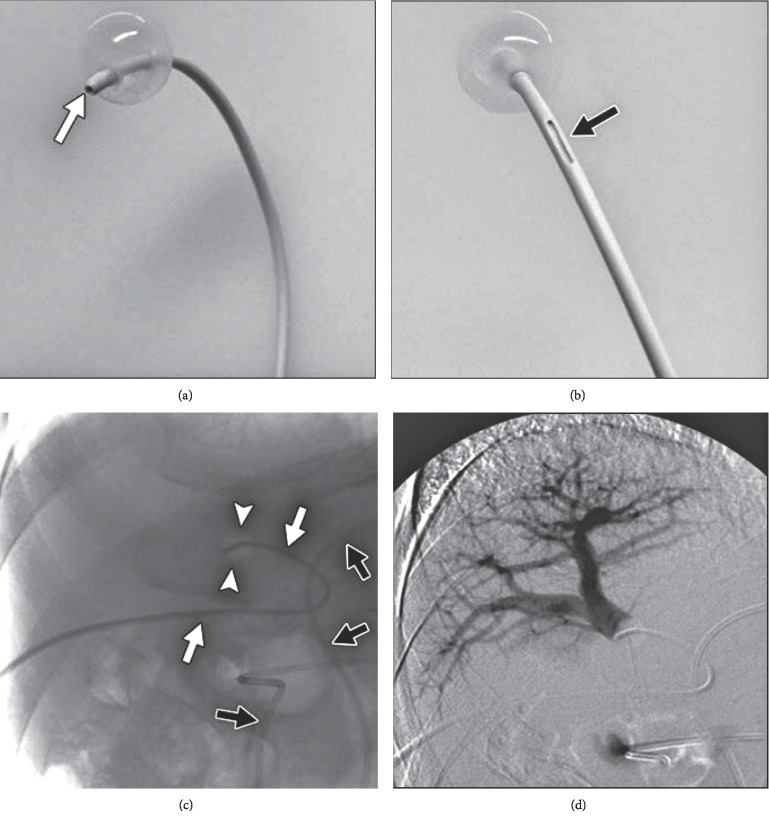
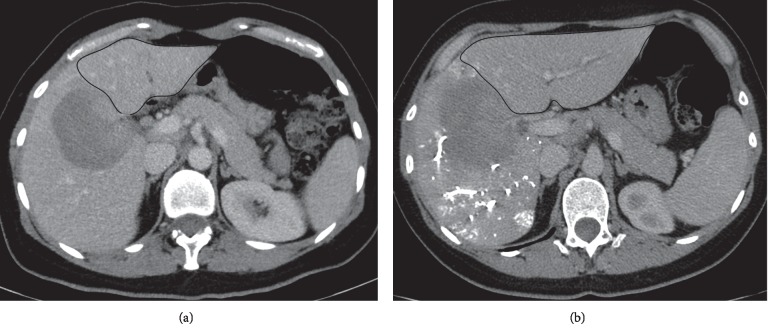
Liver volume and function after hepatectomies are directly correlated to postoperative complications and mortality. Consequently contemporary liver surgery has focused on reaching an adequate future liver remnant so as to diminish postoperative morbidity and mortality. Portal vein embolization has evolved and is the standard of care as a liver regenerative strategy in many surgery departments worldwide before major liver resections. Different embolic materials have been used for portal vein embolization including gelfoam, ethanol, polyvinyl-alcohol particles, calibrated microspheres, central vascular plugs, coils, n-butyl-cyanoacrylate glue, fibrin glue, polidocanol-foam, alcoholic prolamin solution, and ethylene vinyl alcohol copolymer, as sole occluders or in varied combinations. While to date there has been no prospective controlled trial comparing the efficacy of different embolic materials in portal vein embolization, retrospective data insinuates that the use of n-butyl-cyanoacrylate and absolute ethanol produces higher contralateral liver hypertrophies. In this review, we evaluated publications up to August 2019 to assess the technical and regenerative results of portal vein embolization accomplished with different embolic materials. Special attention was given to specific aspects, advantages, and drawbacks of each embolic agent used for portal vein embolization, its liver regenerative performance, and its influence on patient outcome.
Copyright © 2020 Jose Hugo M. Luz et al.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Pamecha V., Glantzounis G., Davies N., Fusai G., Sharma D., Davidson B. Long-term survival and disease recurrence following portal vein embolisation prior to major hepatectomy for colorectal metastases. Annals of Surgical Oncology. 2009;16(5):1202–1207. doi: 10.1245/s10434-008-0269-4. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
