

The Interactive Web-Based Program MSmonitor for Self-Management and Multidisciplinary Care in Persons With Multiple Sclerosis: Quasi-Experimental Study of Short-Term Effects on Patient Empowerment
- PMID: 32149713
- PMCID: PMC7091023
- DOI: 10.2196/14297
The Interactive Web-Based Program MSmonitor for Self-Management and Multidisciplinary Care in Persons With Multiple Sclerosis: Quasi-Experimental Study of Short-Term Effects on Patient Empowerment
Abstract
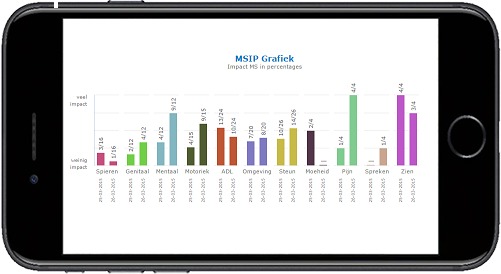
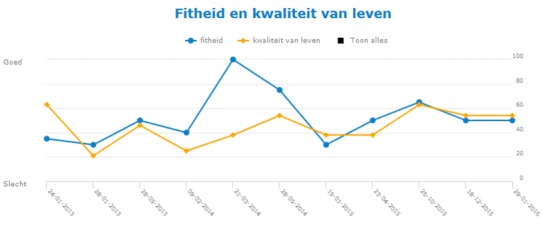
Background: Empowerment helps persons with a chronic disease to self-manage their condition and increase their autonomy and participation. MSmonitor (Curavista bv) is an interactive Web-based program for self-management and multidisciplinary care in multiple sclerosis (MS). It includes, among others, short questionnaires on fatigue (Modified Fatigue Impact Scale-5 [MFIS-5]) and health-related quality of life (HRQoL, Leeds Multiple Sclerosis Quality of Life [LMSQoL]); long questionnaires on disabilities, perception of disabilities (Multiple Sclerosis Impact Profile), and HRQoL (Multiple Sclerosis Quality of Life-54); a Medication and Adherence Inventory and an Activity Diary. The combination MFIS-5, LMSQoL, and Medication and Adherence Inventory constitutes the Quick Scan.
Objective: This study aimed to investigate the short-term effects of MSmonitor on empowerment in patients with MS.
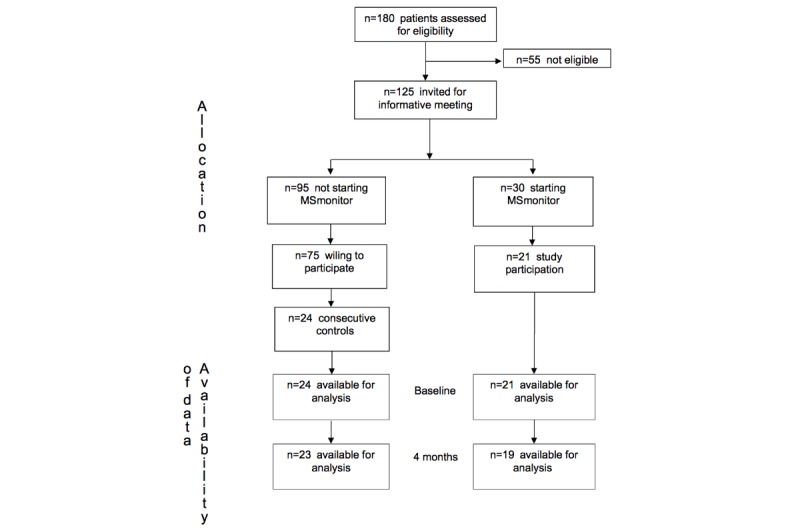
Methods: We conducted a quasi-experimental study in a general hospital. Of the 180 patients with MS, 125 were eligible, 30 used MSmonitor, and 21 participated in the study (mean age 45.4 years, SD 10.2 years). A total of 24 eligible patients who did not use MSmonitor constituted the control group (mean age 49.3 years, SD 11.4 years). At baseline and at 4 months, we assessed self-efficacy (Multiple Sclerosis Self-Efficacy Scale [MSSES]), participation and autonomy (Impact on Participation and Autonomy [IPA] questionnaire), and self-management (Partners In Health [PIH] questionnaire). Differences between time points and groups were tested with paired t tests and χ² tests.
Results: In the MSmonitor group, follow-up values remained unchanged for MSSES control (P=.19), MSSES function (P=.62), IPA limitations (P=.26), IPA problems (P=.40), PIH recognition and management of symptoms (P=.52), PIH adherence to treatment (P=.80), and PIH coping (P=.73), whereas the PIH knowledge score had improved (mean 27.8, SD 1.7 vs mean 28.7, SD 2.0; P=.02). The overall utilization rate of the program components was 83% and that of the Quick Scan was 95%. In the control group, all outcomes had remained unchanged.
Conclusions: The results suggest that for first-time users of the MSmonitor program and their health care providers, it may not be justified to expect a short-term improvement in empowerment in terms of self-efficacy, self-management, autonomy, or participation. Furthermore, a lack of effect on empowerment is not because of nonusage of the program components.
Keywords: eHealth; empowerment; internet-based communication; internet-based intervention; multiple sclerosis; personal autonomy; self-efficacy; self-management; social participation.
©Peter Joseph Joseph Jongen, Gezien ter Veen, Wim Lemmens, Rogier Donders, Esther van Noort, Esther Zeinstra. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 09.03.2020.
Conflict of interest statement
Conflicts of Interest: EN is co-owner of Curavista bv, Geertruidenberg, the Netherlands. PJ has received expense compensation from Curavista bv for serving as chairman of the board of the MSmonitor Foundation, and honoraria from Bayer Netherlands for consultancy activities.
Figures
Similar articles
-
MSmonitor-plus program and video calling care (MPVC) for multidisciplinary care and self-management in multiple sclerosis: study protocol of a single-center randomized, parallel-group, open label, non-inferiority trial.BMC Neurol. 2022 Nov 12;22(1):423. doi: 10.1186/s12883-022-02948-z. BMC Neurol. 2022. PMID: 36371162 Free PMC article.
-
The interactive web-based program MSmonitor for self-management and multidisciplinary care in multiple sclerosis: concept, content, and pilot results.Patient Prefer Adherence. 2015 Dec 11;9:1741-50. doi: 10.2147/PPA.S93783. eCollection 2015. Patient Prefer Adherence. 2015. PMID: 26715841 Free PMC article.
-
A prospective web-based patient-centred interactive study of long-term disabilities, disabilities perception and health-related quality of life in patients with multiple sclerosis in The Netherlands: the Dutch Multiple Sclerosis Study protocol.BMC Neurol. 2015 Aug 4;15:128. doi: 10.1186/s12883-015-0379-0. BMC Neurol. 2015. PMID: 26238866 Free PMC article.
-
The Use and Effects of Electronic Health Tools for Patient Self-Monitoring and Reporting of Outcomes Following Medication Use: Systematic Review.J Med Internet Res. 2018 Dec 18;20(12):e294. doi: 10.2196/jmir.9284. J Med Internet Res. 2018. PMID: 30563822 Free PMC article.
-
Global, regional and national quality of life in patients with multiple sclerosis: a global systematic review and meta-analysis.BMJ Support Palliat Care. 2022 Jun;12(2):158-166. doi: 10.1136/bmjspcare-2020-002604. Epub 2020 Sep 22. BMJ Support Palliat Care. 2022. PMID: 32963057
Cited by
-
Current Implementation of Digital Health in Chronic Disease Management: Scoping Review.J Med Internet Res. 2024 Dec 12;26:e53576. doi: 10.2196/53576. J Med Internet Res. 2024. PMID: 39666972 Free PMC article.
-
Creating a Digital Toolkit to Reduce Fatigue and Promote Quality of Life in Multiple Sclerosis: Participatory Design and Usability Study.JMIR Form Res. 2021 Dec 9;5(12):e19230. doi: 10.2196/19230. JMIR Form Res. 2021. PMID: 34889744 Free PMC article.
-
MSmonitor-plus program and video calling care (MPVC) for multidisciplinary care and self-management in multiple sclerosis: study protocol of a single-center randomized, parallel-group, open label, non-inferiority trial.BMC Neurol. 2022 Nov 12;22(1):423. doi: 10.1186/s12883-022-02948-z. BMC Neurol. 2022. PMID: 36371162 Free PMC article.
-
Evaluating the Utility of Smartphone-Based Sensor Assessments in Persons With Multiple Sclerosis in the Real-World Using an App (elevateMS): Observational, Prospective Pilot Digital Health Study.JMIR Mhealth Uhealth. 2020 Oct 27;8(10):e22108. doi: 10.2196/22108. JMIR Mhealth Uhealth. 2020. PMID: 33107827 Free PMC article.
-
The effect of patient-centered empowerment program through telenursing on self-management in people with multiple sclerosis: a double-blinded randomized clinical trial.BMC Neurol. 2025 Apr 2;25(1):138. doi: 10.1186/s12883-025-04148-x. BMC Neurol. 2025. PMID: 40175934 Free PMC article. Clinical Trial.
References
-
- Rappaport J. Community psychology. In: Corsini R, editor. Encyclopedia of Psychology. New York: Wiley; 1984. pp. 252–254.
-
- Anderson RM, Funnell MM. Patient empowerment: myths and misconceptions. Patient Educ Couns. 2010 Jun;79(3):277–82. doi: 10.1016/j.pec.2009.07.025. http://europepmc.org/abstract/MED/19682830 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
