

TYK2 inhibition reduces type 3 immunity and modifies disease progression in murine spondyloarthritis
- PMID: 32149730
- PMCID: PMC7108927
- DOI: 10.1172/JCI126567
TYK2 inhibition reduces type 3 immunity and modifies disease progression in murine spondyloarthritis
Abstract
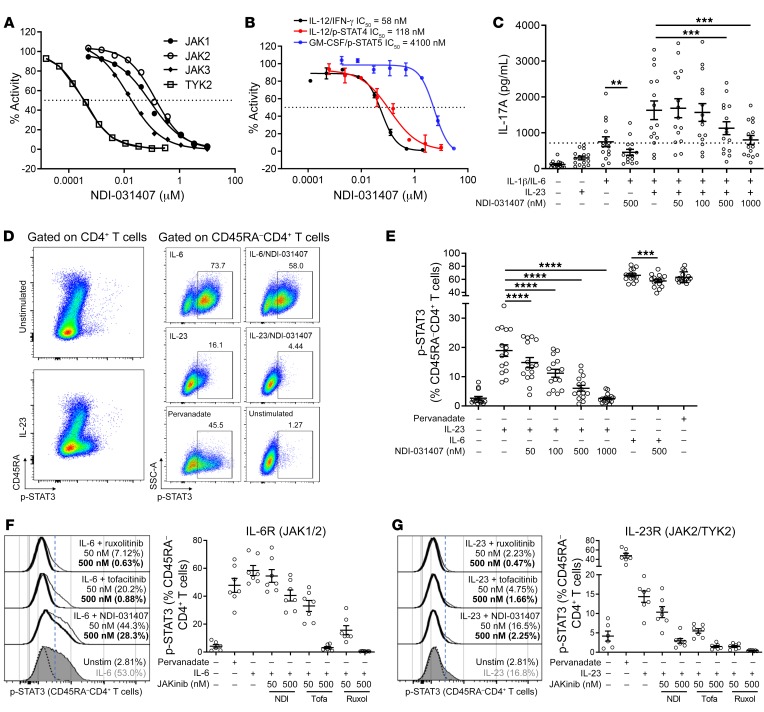
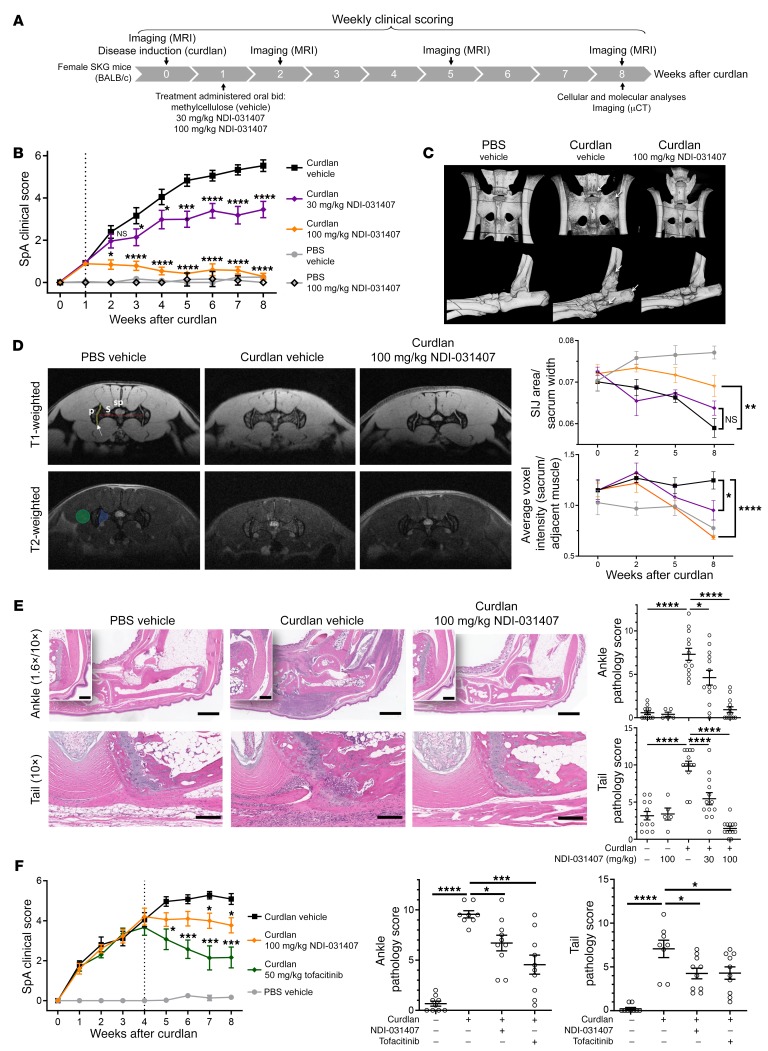
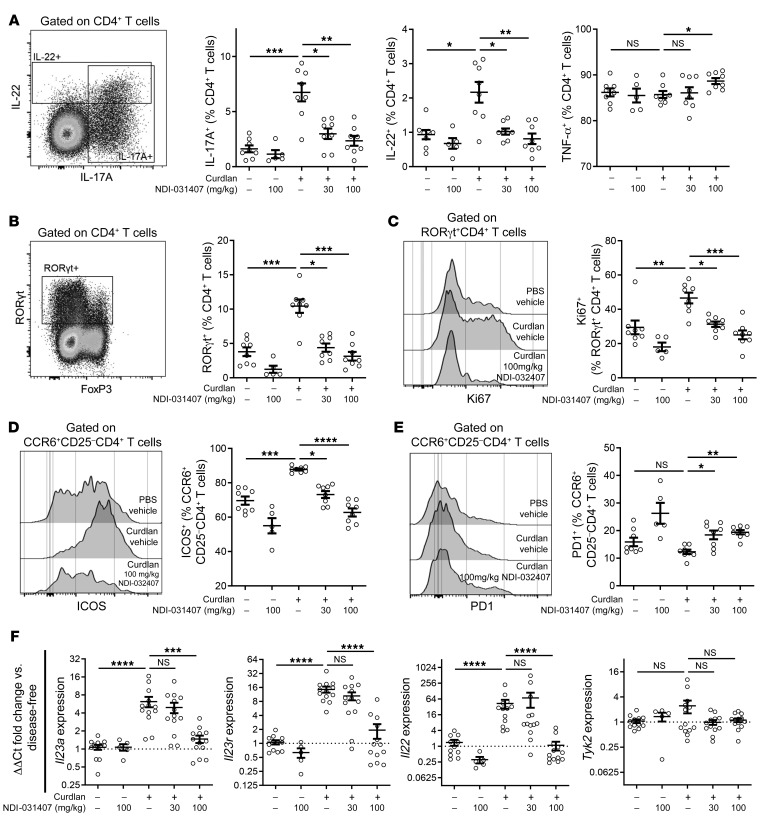
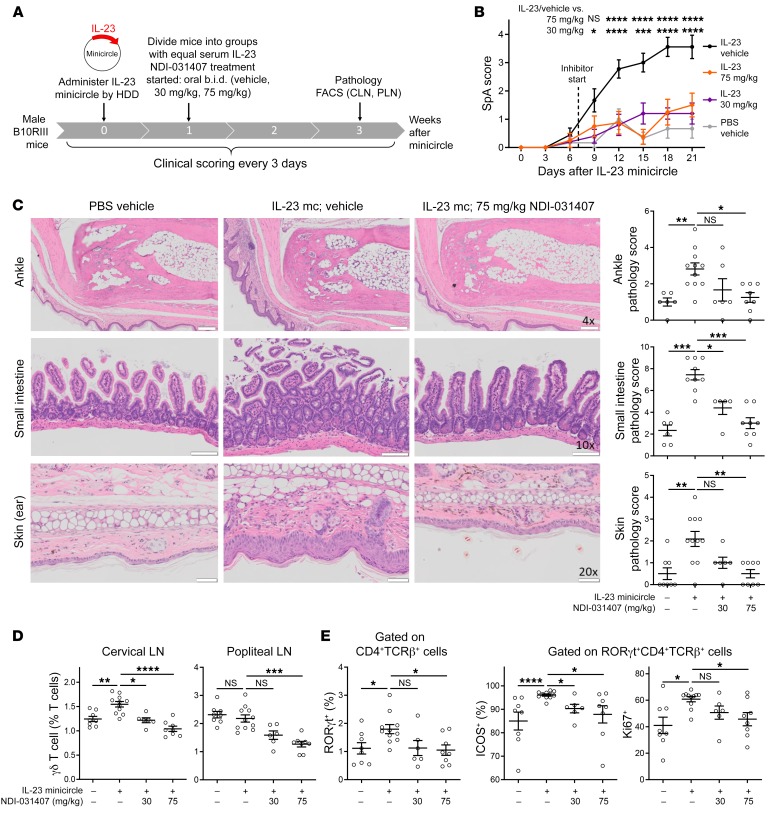
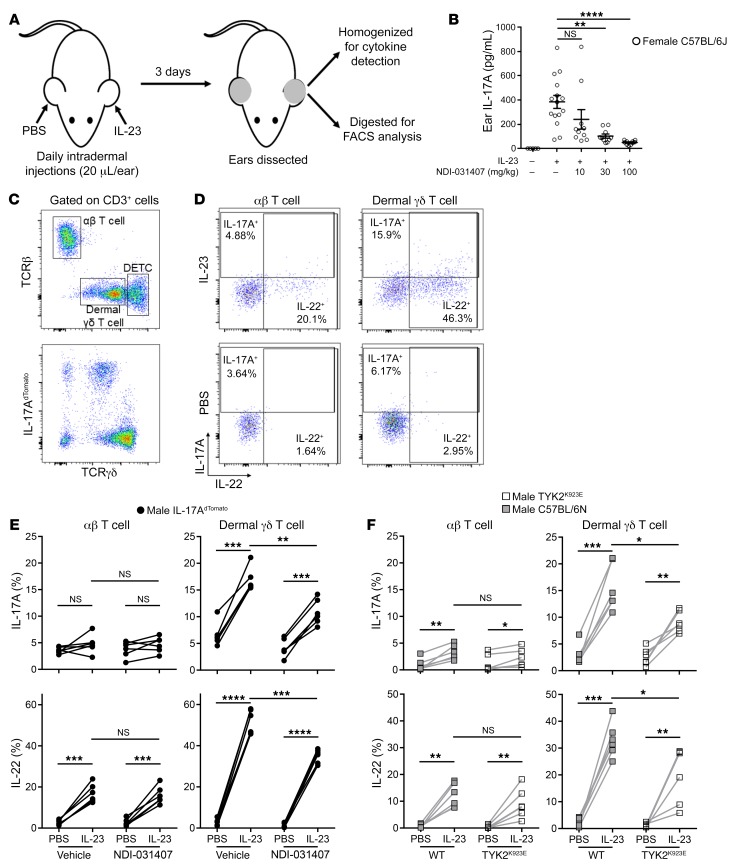
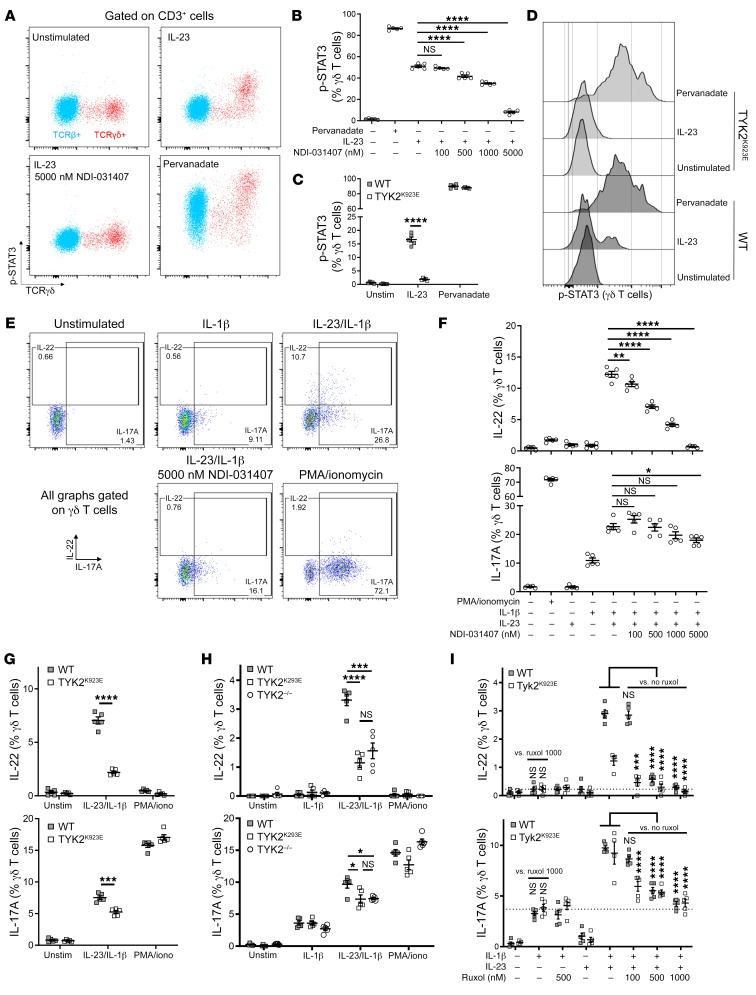
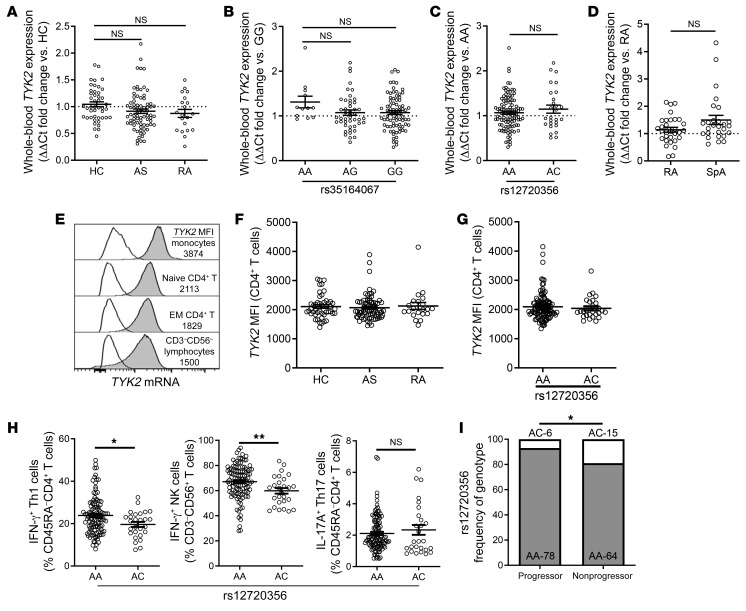
Spondyloarthritis (SpA) represents a family of inflammatory diseases of the spine and peripheral joints. Ankylosing spondylitis (AS) is the prototypic form of SpA in which progressive disease can lead to fusion of the spine. Therapeutically, knowledge of type 3 immunity has translated into the development of IL-23- and IL-17A-blocking antibodies for the treatment of SpA. Despite being able to provide symptomatic control, the current biologics do not prevent the fusion of joints in AS patients. Thus, there is an unmet need for disease-modifying drugs. Genetic studies have linked the Janus kinase TYK2 to AS. TYK2 is a mediator of type 3 immunity through intracellular signaling of IL-23. Here, we describe and characterize a potentially novel small-molecule inhibitor of TYK2 that blocked IL-23 signaling in vitro and inhibited disease progression in animal models of SpA. The effect of the inhibitor appears to be TYK2 specific, using TYK2-inactive mice, which further revealed a duality in the induction of IL-17A and IL-22 by IL-23. Specifically, IL-22 production was TYK2/JAK2/STAT3 dependent, while IL-17A was mostly JAK2 dependent. Finally, we examined the effects of AS-associated TYK2 SNPs on TYK2 expression and function and correlated them with AS disease progression. This work provides evidence that TYK2 inhibitors have great potential as an orally delivered therapeutic for SpA.
Keywords: Arthritis; Autoimmunity; Cytokines; T cells; Therapeutics.
Conflict of interest statement
Figures
Comment in
-
TYK2 inhibition halts SpA.Nat Rev Rheumatol. 2020 May;16(5):248. doi: 10.1038/s41584-020-0417-1. Nat Rev Rheumatol. 2020. PMID: 32231302 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
