

Cost-effectiveness Evaluation of Targeted Surgical and Endoscopic Therapies for Early Colorectal Adenocarcinoma Based on Biomarker Profiles
- PMID: 32150269
- PMCID: PMC7063501
- DOI: 10.1001/jamanetworkopen.2019.19963
Cost-effectiveness Evaluation of Targeted Surgical and Endoscopic Therapies for Early Colorectal Adenocarcinoma Based on Biomarker Profiles
Abstract
Importance: Colorectal cancer (CRC) is the second leading cause of cancer-related mortality in the United States. The prognosis for patients with CRC varies widely, but new prognostic biomarkers provide the opportunity to implement a more individualized approach to treatment selection.
Objective: To assess the cost-effectiveness of 3 therapeutic strategies, namely, endoscopic therapy (ET), laparoscopic colectomy (LC), and open colectomy (OC), for patients with T1 CRC with biomarker profiles that prognosticate varying levels of tumor progression in the US payer perspective.
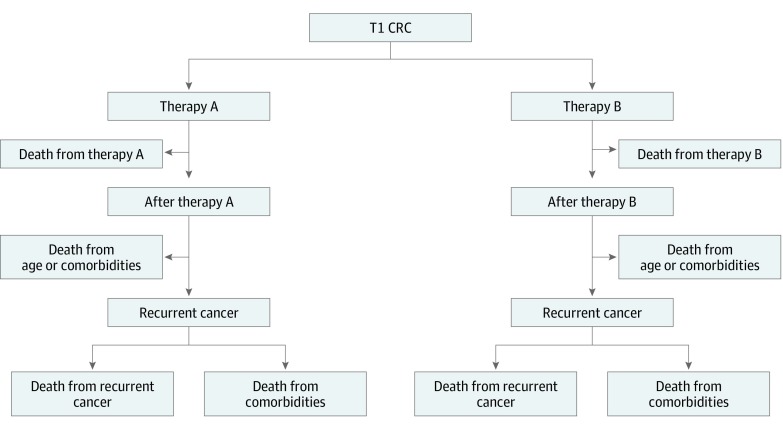
Design, setting, and participants: In this economic evaluation study, a Markov model was developed for the cost-effectiveness analysis. Risks of all-cause mortality and recurrent cancer after ET, LC, or OC were estimated with a 35-year time horizon. Quality of life was based on EuroQoL 5 Dimensions scores reported in the published literature. Hospital and treatment costs reflected Medicare reimbursement rates. Deterministic and probabilistic sensitivity analyses were performed. Data from patients with T1 CRC and 6 biomarker profiles that included adenomatous polyposis coli (APC), TP53 and/or KRAS, or BRAFV600E were used as inputs for the model. Data analyses were conducted from February 27, 2019, to May 13, 2019.
Exposures: Endoscopic therapy, LC, and OC.
Main outcomes and measures: The primary outcomes were unadjusted life-years, quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER) between competing treatment strategies.
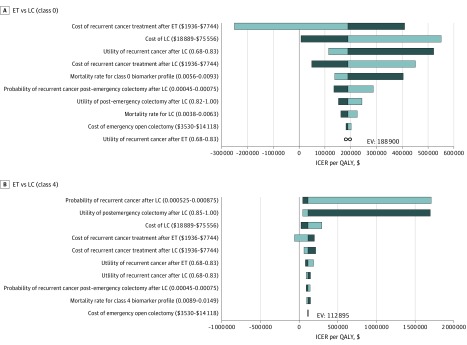
Results: Endoscopic therapy had the highest QALYs and the lowest cost and was the dominant treatment strategy for T1 CRC with the following biomarker profiles: BRAFV600E, APC(1)/KRAS/TP53, APC(2) or APC(2)/KRAS or APC(2)/TP53, or APC(1) or APC(1)/KRAS or APC(1)/TP53. The QALYs gained ranged from 16.97 to 17.22, with costs between $68 902.75 and $77 784.53 in these subgroups. For the 2 more aggressive biomarker profiles with worse prognoses (APC(2)/KRAS/TP53 and APCwt [wild type]), LC was the most effective strategy (with 16.45 and 16.61 QALYs gained, respectively) but was not cost-effective. Laparoscopic colectomy cost $65 234.87 for APC(2)/KRAS/TP53 and $71 250.56 for APCwt, resulting in ICERs of $113 290 per QALY and $178 765 per QALY, respectively.
Conclusions and relevance: This modeling analysis found that ET was the most effective strategy for patients with T1 CRC with less aggressive biomarker profiles. For patients with more aggressive profiles, LC was more effective but was costly, rendering ET the cost-effective option. This study highlights the potential utility of prognostic biomarkers in T1 CRC treatment selection.
Conflict of interest statement
Figures
Comment in
-
Assessment of Treatment Cost-effectiveness Using a Colorectal Cancer Mutation Profile.JAMA Netw Open. 2020 Mar 2;3(3):e1919991. doi: 10.1001/jamanetworkopen.2019.19991. JAMA Netw Open. 2020. PMID: 32150267 No abstract available.
Similar articles
-
Cost-effectiveness of Maintenance Capecitabine and Bevacizumab for Metastatic Colorectal Cancer.JAMA Oncol. 2019 Feb 1;5(2):236-242. doi: 10.1001/jamaoncol.2018.5070. JAMA Oncol. 2019. PMID: 30489611 Free PMC article.
-
Prospective cost-effectiveness analysis of cetuximab in metastatic colorectal cancer: evaluation of National Cancer Institute of Canada Clinical Trials Group CO.17 trial.J Natl Cancer Inst. 2009 Sep 2;101(17):1182-92. doi: 10.1093/jnci/djp232. Epub 2009 Aug 7. J Natl Cancer Inst. 2009. PMID: 19666851
-
Contrasting Effectiveness and Cost-Effectiveness of Colorectal Cancer Screening Under Commercial Insurance vs. Medicare.Am J Gastroenterol. 2018 Dec;113(12):1836-1847. doi: 10.1038/s41395-018-0106-8. Epub 2018 Jun 15. Am J Gastroenterol. 2018. PMID: 29904156 Free PMC article.
-
Impact of comorbidity on colorectal cancer screening cost-effectiveness study in diabetic populations.J Gen Intern Med. 2012 Jun;27(6):730-8. doi: 10.1007/s11606-011-1972-6. Epub 2012 Jan 12. J Gen Intern Med. 2012. PMID: 22237663 Free PMC article. Review.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.Health Technol Assess. 2007 Dec;11(51):iii-iv, 1-164. doi: 10.3310/hta11510. Health Technol Assess. 2007. PMID: 18021578 Review.
Cited by
-
Bowel function, quality of life, and mental health of patients with high-grade intraepithelial neoplasia or T1 colorectal cancer after organ-preserving versus organ-resection surgeries: a cross-sectional study at a Chinese tertiary care center.Surg Endosc. 2024 Oct;38(10):5756-5768. doi: 10.1007/s00464-024-11120-2. Epub 2024 Aug 14. Surg Endosc. 2024. PMID: 39143332
-
Treatment for T1 colorectal cancers substratified by site and size: "horses for courses".Front Med (Lausanne). 2023 Oct 12;10:1230844. doi: 10.3389/fmed.2023.1230844. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37901402 Free PMC article.
-
The Cost Effectiveness of Genomic Medicine in Cancer Control: A Systematic Literature Review.Appl Health Econ Health Policy. 2025 May;23(3):359-393. doi: 10.1007/s40258-025-00949-w. Epub 2025 Mar 29. Appl Health Econ Health Policy. 2025. PMID: 40172779 Free PMC article.
-
Cost-utility advantage of interventional endoscopy.Surg Endosc. 2023 Feb;37(2):1031-1037. doi: 10.1007/s00464-022-09599-8. Epub 2022 Sep 12. Surg Endosc. 2023. PMID: 36097098
References
-
- Croke L. Colorectal cancer screening: ACS updates guideline for adults with average risk. Am Fam Physician. 2019;99(2):-. - PubMed
-
- National Cancer Institute; Surveillance, Epidemiology, and End Results Program. Cancer stat facts: colorectal cancer. https://seer.cancer.gov/statfacts/html/colorect.html. Accessed December 10, 2019.
-
- Puppa G, Sonzogni A, Colombari R, Pelosi G. TNM staging system of colorectal carcinoma: a critical appraisal of challenging issues. Arch Pathol Lab Med. 2010;134(6):837-852. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
