

Evaluation of cisplatin-induced injury in human kidney organoids
- PMID: 32150447
- PMCID: PMC7395477
- DOI: 10.1152/ajprenal.00597.2019
Evaluation of cisplatin-induced injury in human kidney organoids
Abstract
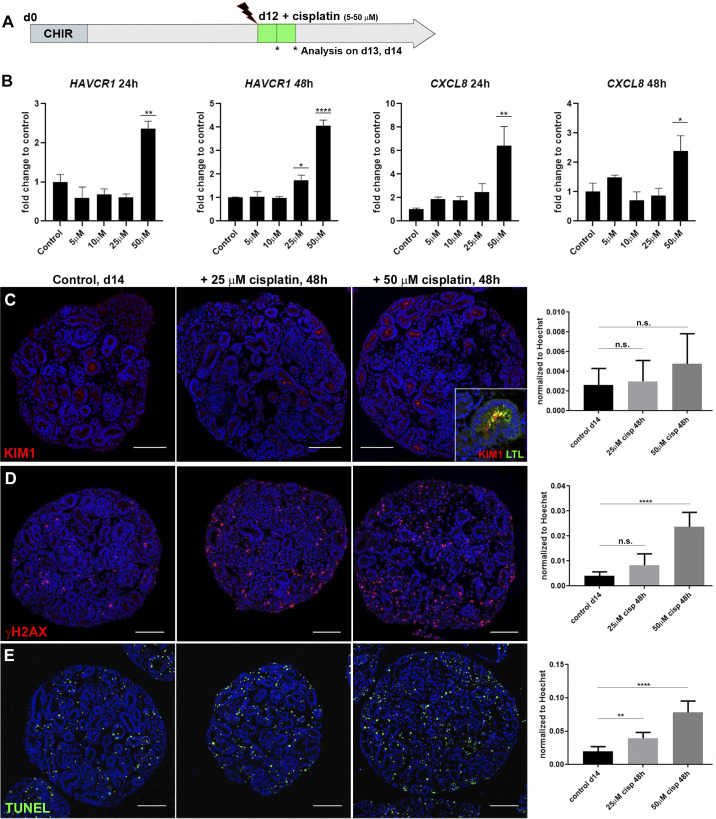
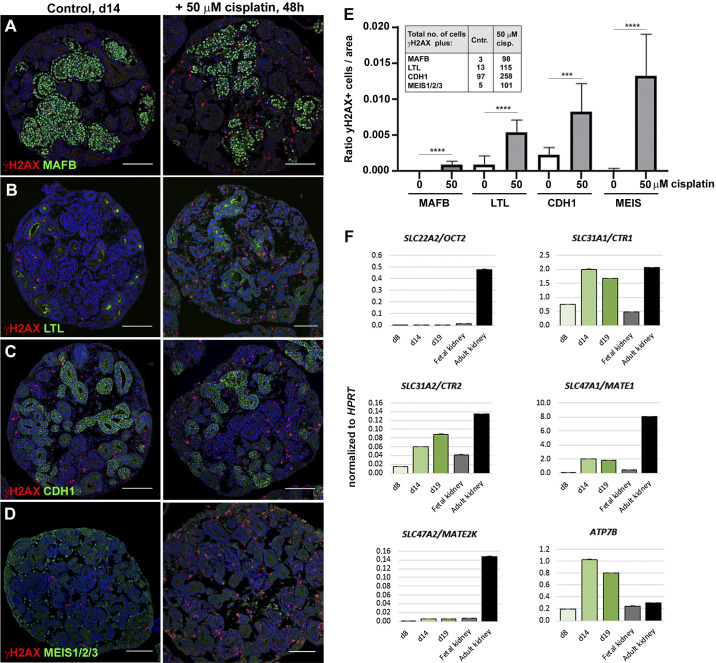
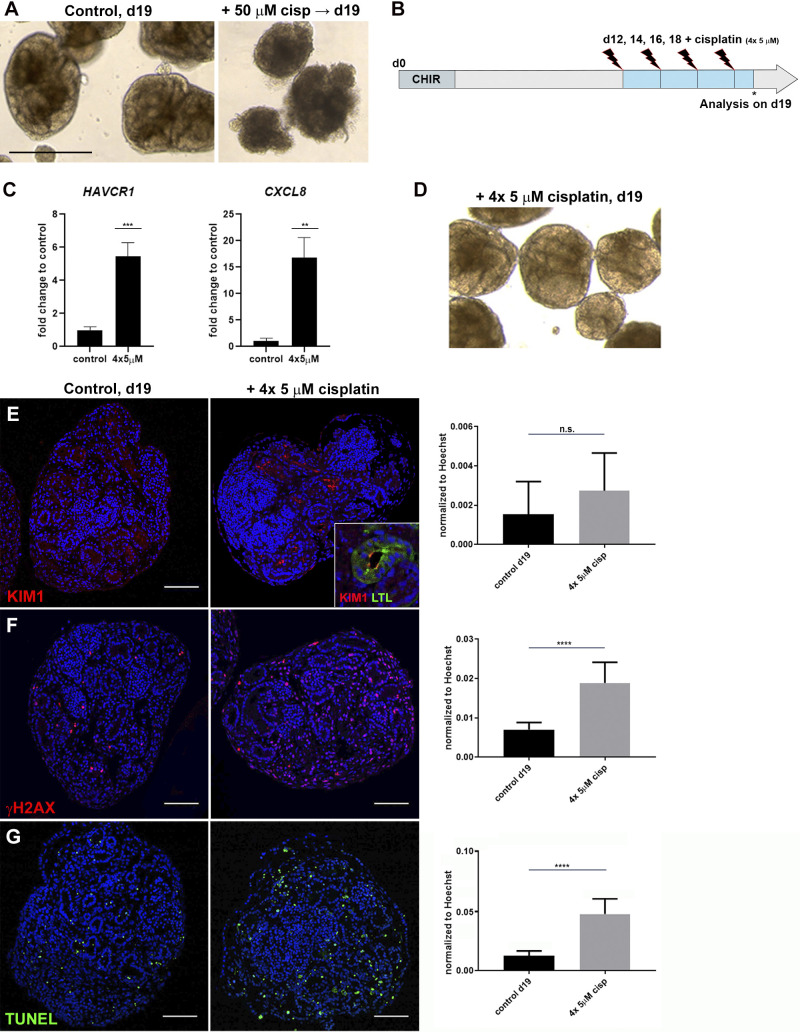
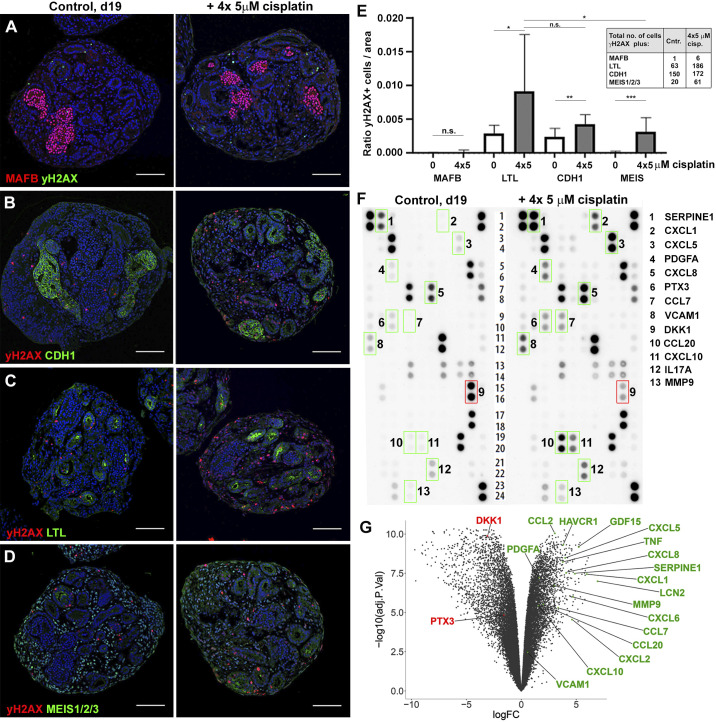
Acute kidney injury (AKI) remains a major global healthcare problem, and there is a need to develop human-based models to study AKI in vitro. Toward this goal, we have characterized induced pluripotent stem cell-derived human kidney organoids and their response to cisplatin, a chemotherapeutic drug that induces AKI and preferentially damages the proximal tubule. We found that a single treatment with 50 µM cisplatin induces hepatitis A virus cellular receptor 1 (HAVCR1) and C-X-C motif chemokine ligand 8 (CXCL8) expression, DNA damage (γH2AX), and cell death in the organoids but greatly impairs organoid viability. DNA damage was not specific to the proximal tubule but also affected the distal tubule and interstitial cell populations. This lack of specificity correlated with low expression of proximal tubule-specific SLC22A2/organic cation transporter 2 (OCT2) for cisplatin. To improve viability, we developed a repeated low-dose regimen of 4 × 5 µM cisplatin over 7 days and found this caused less toxicity while still inducing a robust injury response that included secretion of known AKI biomarkers and inflammatory cytokines. This work validates the use of human kidney organoids to model aspects of cisplatin-induced injury, with the potential to identify new AKI biomarkers and develop better therapies.
Keywords: acute kidney injury; acute kidney injury biomarker; cisplatin; cytokine; inflammation; kidney organoids; nephrotoxicity; proximal tubule; repeated low-dose regimen.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Freedman BS, Brooks CR, Lam AQ, Fu H, Morizane R, Agrawal V, Saad AF, Li MK, Hughes MR, Werff RV, Peters DT, Lu J, Baccei A, Siedlecki AM, Valerius MT, Musunuru K, McNagny KM, Steinman TI, Zhou J, Lerou PH, Bonventre JV. Modelling kidney disease with CRISPR-mutant kidney organoids derived from human pluripotent epiblast spheroids. Nat Commun 6: 8715, 2015. doi: 10.1038/ncomms9715. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases