

Diagnostic Accuracy of Videofluoroscopy for Symptomatic Cervical Spine Injury Following Whiplash Trauma
- PMID: 32150926
- PMCID: PMC7084423
- DOI: 10.3390/ijerph17051693
Diagnostic Accuracy of Videofluoroscopy for Symptomatic Cervical Spine Injury Following Whiplash Trauma
Abstract
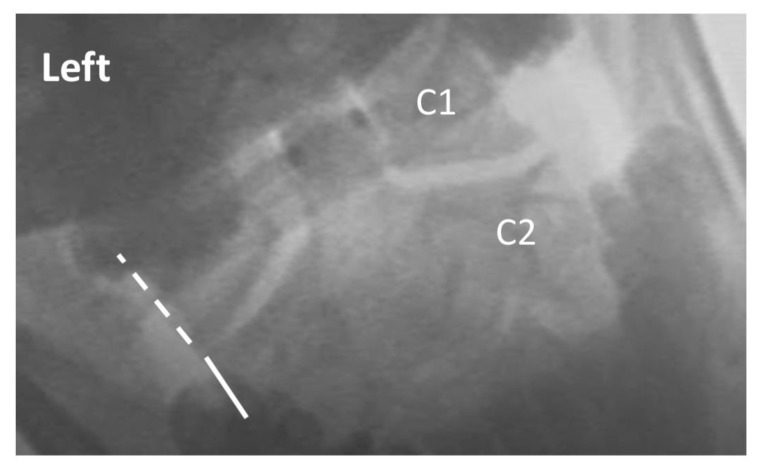
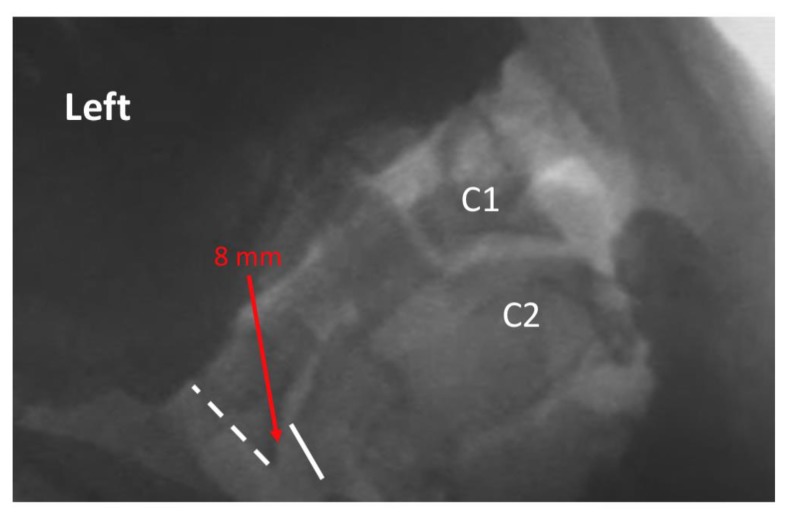
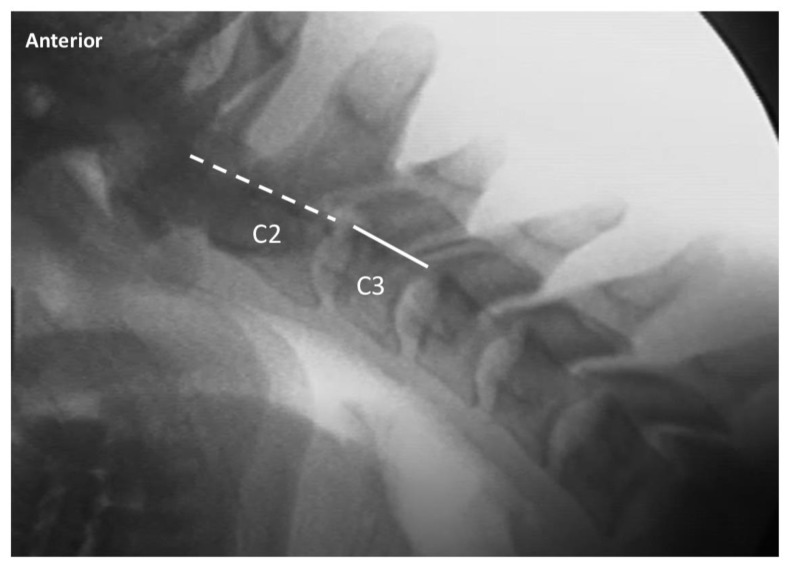
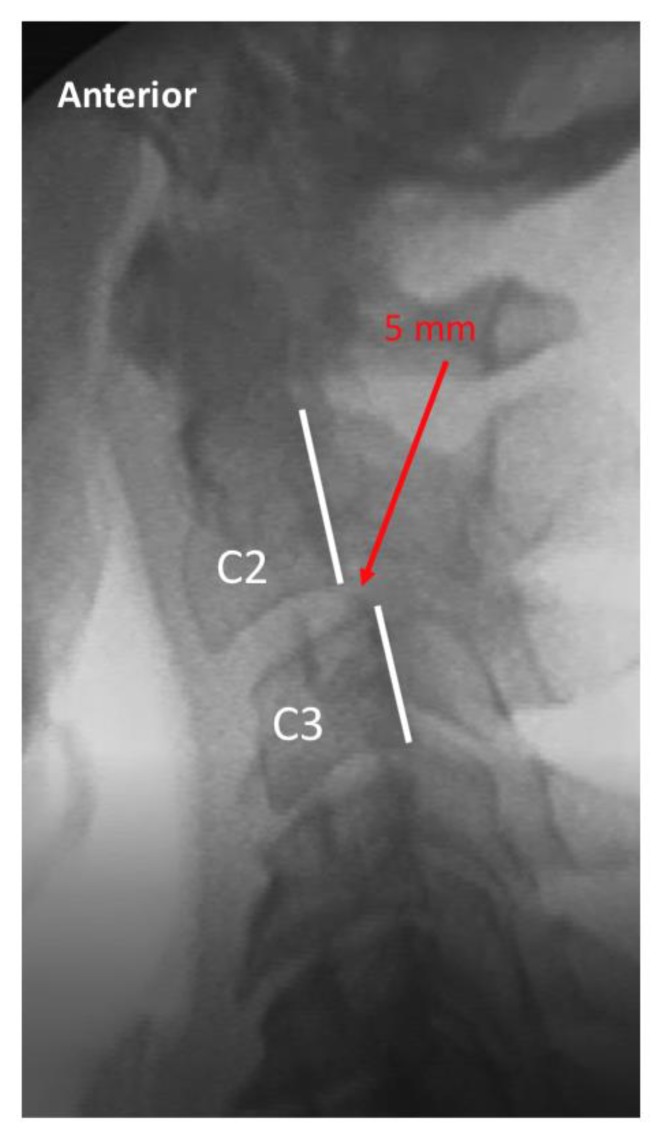
Background: Intervertebral instability is a relatively common finding among patients with chronic neck pain after whiplash trauma. Videofluoroscopy (VF) of the cervical spine is a potentially sensitive diagnostic tool for evaluating instability, as it offers the ability to examine relative intervertebral movement over time, and across the entire continuum of voluntary movement of the patient. At the present time, there are no studies of the diagnostic accuracy of VF for discriminating between injured and uninjured populations.
Methods: Symptomatic (injured) study subjects were recruited from consecutive patients with chronic (>6 weeks) post-whiplash pain presenting to medical and chiropractic offices equipped with VF facilities. Asymptomatic (uninjured) volunteers were recruited from family and friends of patients. An ethical review and oversight were provided by the Spinal Injury Foundation, Broomfield, CO. Three statistical models were utilized to assess the sensitivity, specificity, positive and negative predictive values (PPV and NPV) of positive VF findings to correctly discriminate between injured and uninjured subjects.
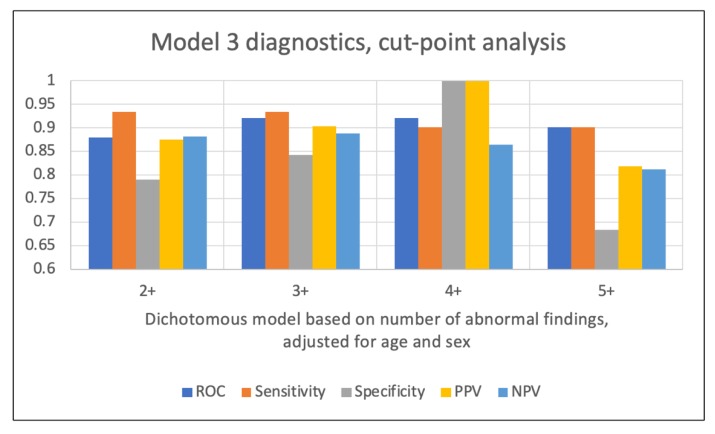
Results: A total of 196 subjects (119 injured, 77 uninjured) were included in the study. All three statistical models demonstrated high levels of sensitivity and specificity (i.e., receiver operating characteristic (ROC) values of 0.71 to 0.95), however, the model with the greatest practical clinical utility was based on the number of abnormal VF findings. For 2+ abnormal VF findings, the ROC was 0.88 (93% sensitivity, 79% specificity) and the PPV and NPV were both 88%. The highest PPV (1.0) was observed with 4+ abnormal findings.
Conclusions: Videofluoroscopic examination of the cervical spine provides a high degree of diagnostic accuracy for the identification of vertebral instability in patients with chronic pain stemming from whiplash trauma.
Keywords: digital motion x-ray; instability; positive predictive value; videofluoroscopy; whiplash.
Conflict of interest statement
Author M.D.F. provides medicolegal consulting services. The remaining authors declare no conflict of interest.
Figures
References
-
- Nolet P.S., Emary P.C., Kristman V.L., Murnaghan K., Zeegers M.P., Freeman M.D. Exposure to a Motor Vehicle Collision and the Risk of Future Neck Pain: A Systematic Review and Meta-Analysis. PM&R. [(accessed on 12 June 2019)]; Available online: http://www.ncbi.nlm.nih.gov/pubmed/31020768. - PMC - PubMed
-
- Insurance Research Council . Auto Injury Insurance Claims: Countrywide Patterns in Treatment, Cost, and Compensation. Insurance Research Council; Malvern, PA, USA: 2008.
-
- McConnell W.E., Howard R.P., Guzman H.M., Bomar J.B., Raddin J.H., Benedict J.V., Smith H.L., Hatsell C.P. SAE Technical Paper 930889. SAE International; Warrendale, PA, USA: 1993. Analysis of Human Test Subject Kinematic Responses to Low Velocity Rear End Impacts.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
