

Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer
- PMID: 32150938
- PMCID: PMC7139727
- DOI: 10.3390/cancers12030595
Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer
Abstract
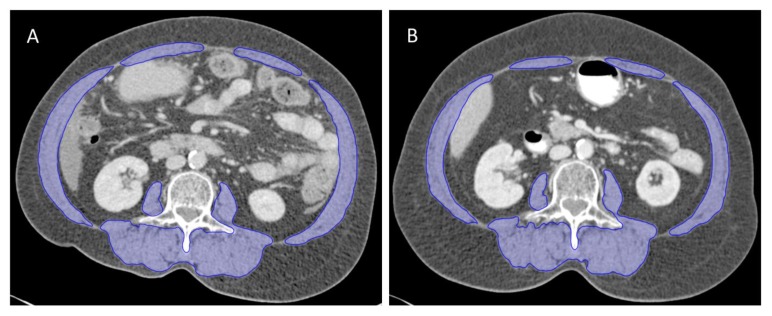
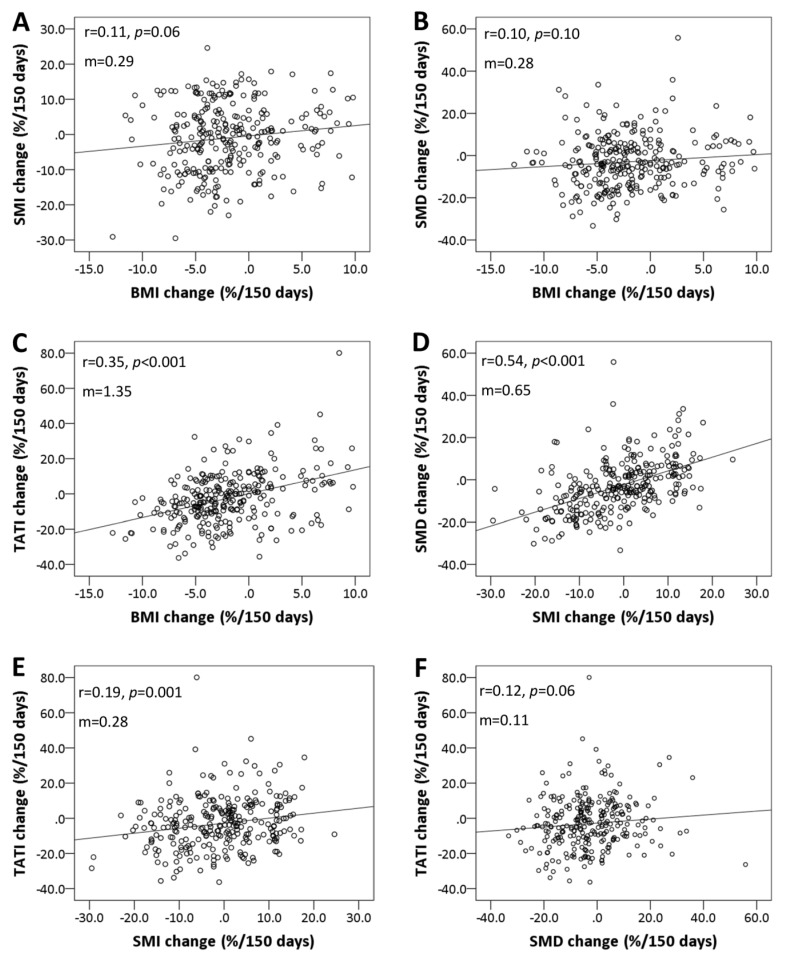
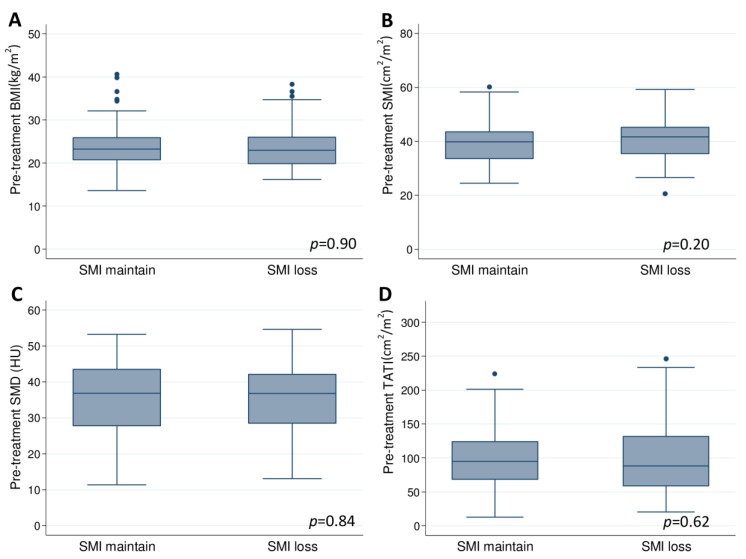
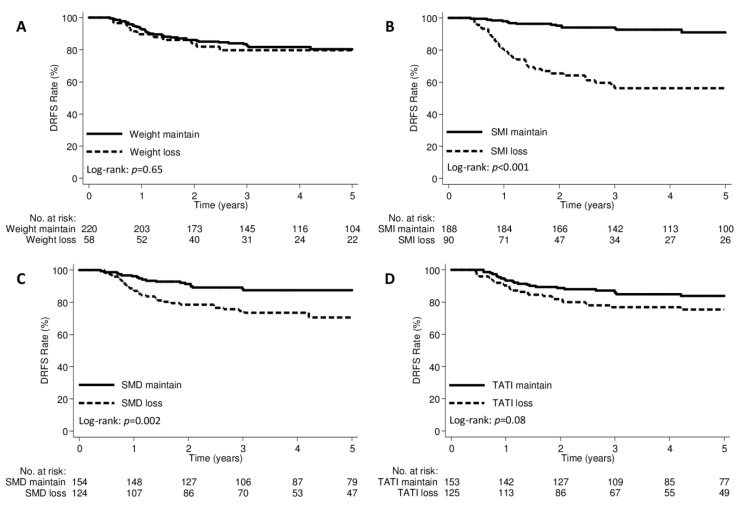
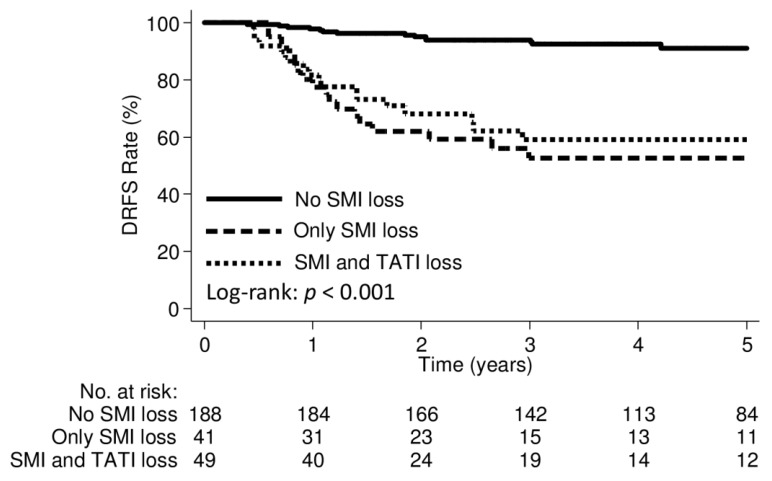
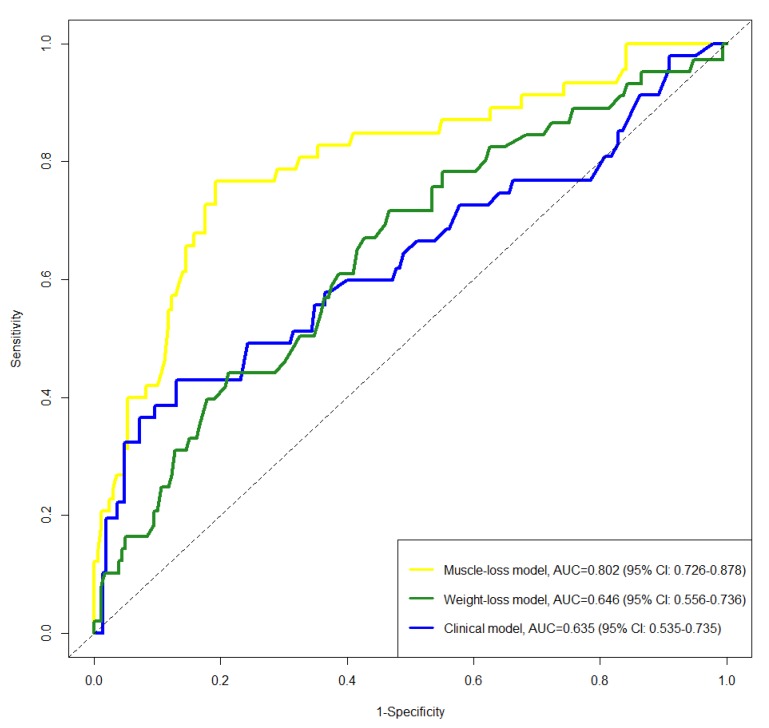
This study aimed to evaluate whether computed tomography (CT)-based muscle measurement predicts distant failure in patients with locally advanced cervical cancer (LACC). Data from 278 patients with LACC who underwent chemoradiation therapy (CCRT) between 2004 and 2017 were analysed. Changes in the skeletal muscle index (SMI), skeletal muscle density, and total adipose tissue index during CCRT were calculated from CT images taken at the baseline and after CCRT. The predictive capability of CT-based muscle measurement for distant failure was evaluated using Cox proportional hazards regression, Harrell's concordance index (C-index), and time-dependent receiver operating characteristic curves. SMI loss ≥ 5% was independently associated with worse distant recurrence-free survival (DRFS) (HR: 6.31, 95% CI: 3.18-12.53; p < 0.001). The addition of muscle change to clinical models, including International Federation of Gynaecology and Obstetrics (FIGO) stage, lymph nodes, pathology, and squamous cell carcinoma-antigen, achieved higher C-indices (0.824 vs. 0.756; p < 0.001). Models including muscle change had superior C-indices than those including weight change (0.824 vs. 0.758; p < 0.001). The area under the curve for predicting 3-year DRFS was the highest for the muscle-loss model (0.802, muscle-loss model; 0.635, clinical model; and 0.646, weight-loss model). Our study demonstrated that muscle loss after CCRT was independently associated with worse DRFS and that integrating muscle loss into models including classical prognostic factors improved the prediction of distant failure.
Keywords: cervical cancer; chemoradiotherapy; computed tomography; distant failures; skeletal muscle loss.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Sturdza A., Potter R., Fokdal L.U., Haie-Meder C., Tan L.T., Mazeron R., Petric P., Segedin B., Jurgenliemk-Schulz I.M., Nomden C., et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother. Oncol. 2016;120:428–433. doi: 10.1016/j.radonc.2016.03.011. - DOI - PubMed
-
- Lee J., Lin J.B., Chang C.L., Jan Y.T., Sun F.J., Wu M.H., Chen Y.J. Prophylactic lower para-aortic irradiation using intensity-modulated radiotherapy mitigates the risk of para-aortic recurrence in locally advanced cervical cancer: A 10-year institutional experience. Gynecol. Oncol. 2017;146:20–26. doi: 10.1016/j.ygyno.2017.04.016. - DOI - PubMed
-
- Liang J.A., Chen S.W., Hung Y.C., Yeh L.S., Chang W.C., Lin W.C., Chang Y.Y. Low-dose, prophylactic, extended-field, intensity-modulated radiotherapy plus concurrent weekly cisplatin for patients with stage IB2-IIIB cervical cancer, positive pelvic lymph nodes, and negative para-aortic lymph nodes. Int. J. Gynecol. Cancer. 2014;24:901–907. doi: 10.1097/IGC.0b013e31829f4dc5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
