

Comprehensive Immunoprofiles of Renal Cell Carcinoma Subtypes
- PMID: 32150988
- PMCID: PMC7139472
- DOI: 10.3390/cancers12030602
Comprehensive Immunoprofiles of Renal Cell Carcinoma Subtypes
Abstract
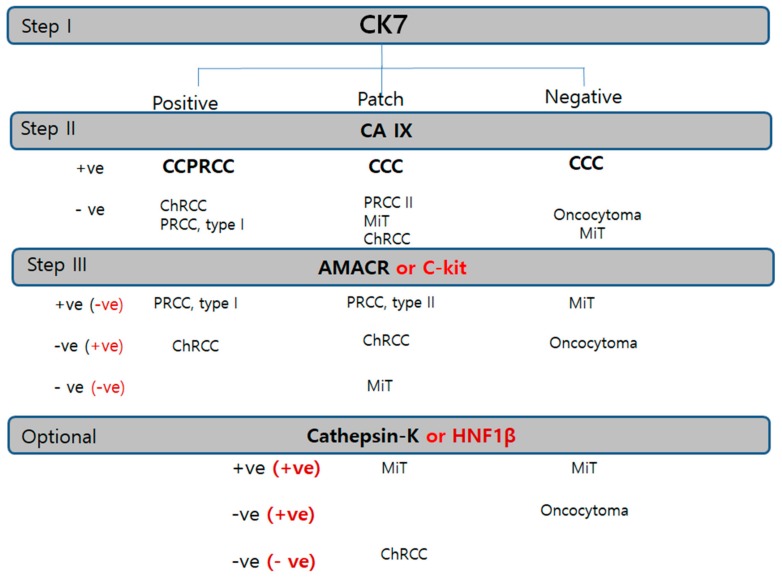
In recent years, renal epithelial tumors have been among the fastest reclassifying tumors, requiring updates to the tumor classification system. Nonetheless, immunohistochemistry (IHC) remains the most widely used tool for renal epithelial tumors. In this proposal, we aimed to create the most efficient IHC panel for categorizing the diverse subtypes of renal tumors, and to find out more specific immunohistochemical results in each subtype or each antibody. A total of 214 renal tumors were analyzed using 10 possible IHC markers to differentiate subtypes, including three major renal cell carcinoma (RCC) subtypes, clear-cell type (50 cases), papillary type (50 cases), and chromophobe type (20 cases), and minor subtypes (MiT RCC, 13 cases; collecting duct carcinoma, 5 cases; and oncocytoma, 10 cases). A triple immunomarker (cytokeratin 7 (CK7)-carbonic anhydrase IX (CAIX)- alpha-methylacyl-CoA racemase (AMACR)) panel is useful in particular high-grade clear-cell tumors. If IHC remains ambiguous, the use of an adjunctive panel can be suggested, including CD10, epithelial membrane antigen, cathepsin K, c-kit, hepatocyte nuclear factor 1-β, and E-cadherin. For an efficient immunohistochemical strategy for subtyping of RCC, we conclude that the CK7-CAIX-AMACR panel is the best primary choice for screening subtyping.
Keywords: Renal cell carcinoma; algorithm; diagnosis; immunohistochemistry; subtyping.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Immunohistochemical panel for differentiating renal cell carcinoma with clear and papillary features.J Microsc Ultrastruct. 2015 Apr-Jun;3(2):68-74. doi: 10.1016/j.jmau.2015.01.003. Epub 2015 Feb 3. J Microsc Ultrastruct. 2015. PMID: 30023184 Free PMC article.
-
Role of immunohistochemistry in the evaluation of needle core biopsies in adult renal cortical tumors: an ex vivo study.Am J Surg Pathol. 2011 Jul;35(7):949-61. doi: 10.1097/PAS.0b013e31821e25cd. Am J Surg Pathol. 2011. PMID: 21677535
-
Role of carbonic anhydrase IX, α-methylacyl coenzyme a racemase, cytokeratin 7, and galectin-3 in the evaluation of renal neoplasms: a tissue microarray immunohistochemical study.Ann Diagn Pathol. 2013 Feb;17(1):58-62. doi: 10.1016/j.anndiagpath.2012.07.002. Epub 2012 Aug 14. Ann Diagn Pathol. 2013. PMID: 22898056
-
Immunohistochemical diagnosis of renal neoplasms.Arch Pathol Lab Med. 2011 Jan;135(1):92-109. doi: 10.5858/2010-0478-RAR.1. Arch Pathol Lab Med. 2011. PMID: 21204715 Review.
-
Recent advances of immunohistochemistry for diagnosis of renal tumors.Pathol Int. 2013 Aug;63(8):381-90. doi: 10.1111/pin.12080. Pathol Int. 2013. PMID: 23957913 Review.
Cited by
-
Clinically Silent, Metastatic Renal Cell Carcinoma Detected on Routine Screening Mammogram: A Report of a Rare Case and Review of Literature.Cureus. 2023 Nov 6;15(11):e48352. doi: 10.7759/cureus.48352. eCollection 2023 Nov. Cureus. 2023. PMID: 38060756 Free PMC article.
-
DDX3X is Epigenetically Repressed in Renal Cell Carcinoma and Serves as a Prognostic Indicator and Therapeutic Target in Cancer Progression.Int J Mol Sci. 2020 Apr 20;21(8):2881. doi: 10.3390/ijms21082881. Int J Mol Sci. 2020. PMID: 32326089 Free PMC article.
-
Prompts to Table: Specification and Iterative Refinement for Clinical Information Extraction with Large Language Models.medRxiv [Preprint]. 2025 Apr 1:2025.02.11.25322107. doi: 10.1101/2025.02.11.25322107. medRxiv. 2025. Update in: NPJ Digit Med. 2025 May 23;8(1):301. doi: 10.1038/s41746-025-01686-z. PMID: 39990557 Free PMC article. Updated. Preprint.
-
Thyroid-like Follicular Carcinoma of the Kidney: The Follicles Are out There in the Kidney-Now What?Diagnostics (Basel). 2025 Apr 27;15(9):1111. doi: 10.3390/diagnostics15091111. Diagnostics (Basel). 2025. PMID: 40361930 Free PMC article.
-
Diagnostic Biomarkers in Renal Cell Tumors According to the Latest WHO Classification: A Focus on Selected New Entities.Cancers (Basel). 2024 May 13;16(10):1856. doi: 10.3390/cancers16101856. Cancers (Basel). 2024. PMID: 38791935 Free PMC article. Review.
References
-
- Lopez-Beltran A., Cheng L., Vidal A., Scarpelli M., Kirkali Z., Blanca A., Montironi R. Pathology of renal cell carcinoma: An update. Anal. Quant. Cytopathol. Histpathol. 2013;35:61–76. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
