

Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): a prospective cohort study
- PMID: 32151332
- PMCID: PMC7473597
- DOI: 10.1016/S1473-3099(19)30755-8
Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): a prospective cohort study
Erratum in
-
Correction to Lancet Infect Dis 2020; published online March 6. https://doi.org/10.1016/S1473-3099(19)30755-8.Lancet Infect Dis. 2020 Jun;20(6):e116. doi: 10.1016/S1473-3099(20)30354-6. Epub 2020 Apr 23. Lancet Infect Dis. 2020. PMID: 32334656 No abstract available.
Abstract
Background: Carbapenem-resistant Enterobacterales (CRE) are a global threat. We aimed to describe the clinical and molecular characteristics of Centers for Disease Control and Prevention (CDC)-defined CRE in the USA.
Methods: CRACKLE-2 is a prospective, multicentre, cohort study. Patients hospitalised in 49 US hospitals, with clinical cultures positive for CDC-defined CRE between April 30, 2016, and Aug 31, 2017, were included. There was no age exclusion. The primary outcome was desirability of outcome ranking (DOOR) at 30 days after index culture. Clinical data and bacteria were collected, and whole genome sequencing was done. This trial is registered with ClinicalTrials.gov, number NCT03646227.
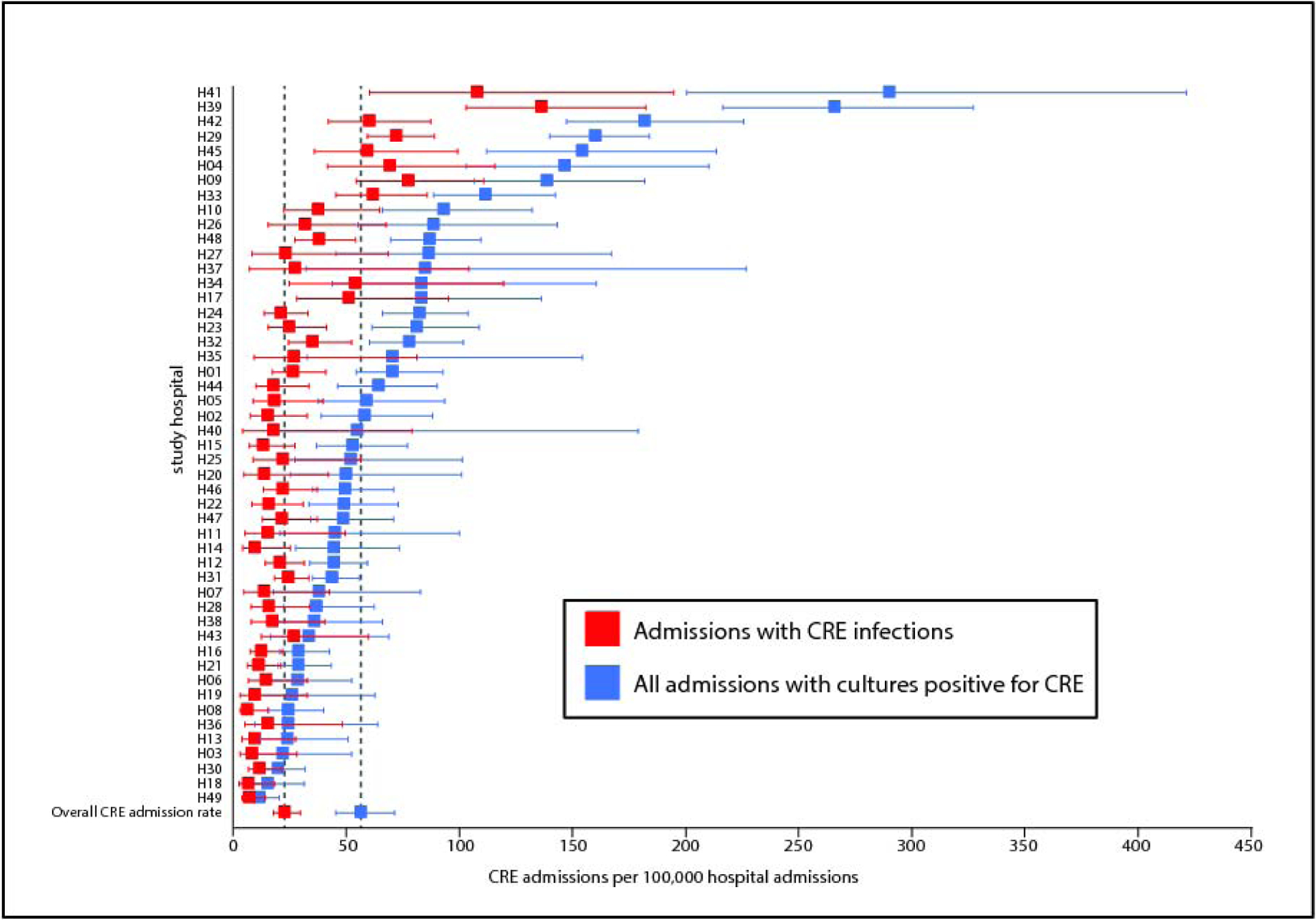
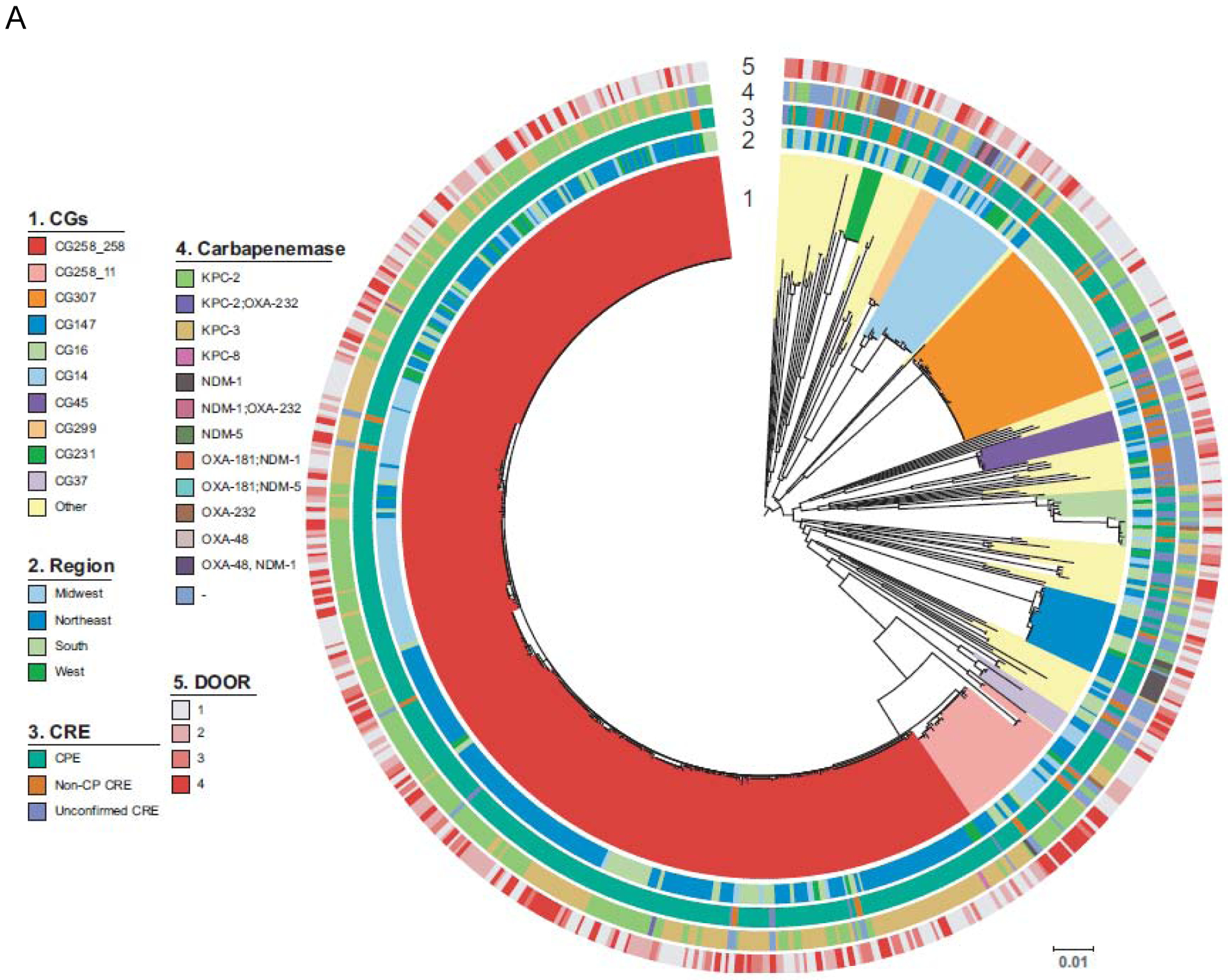
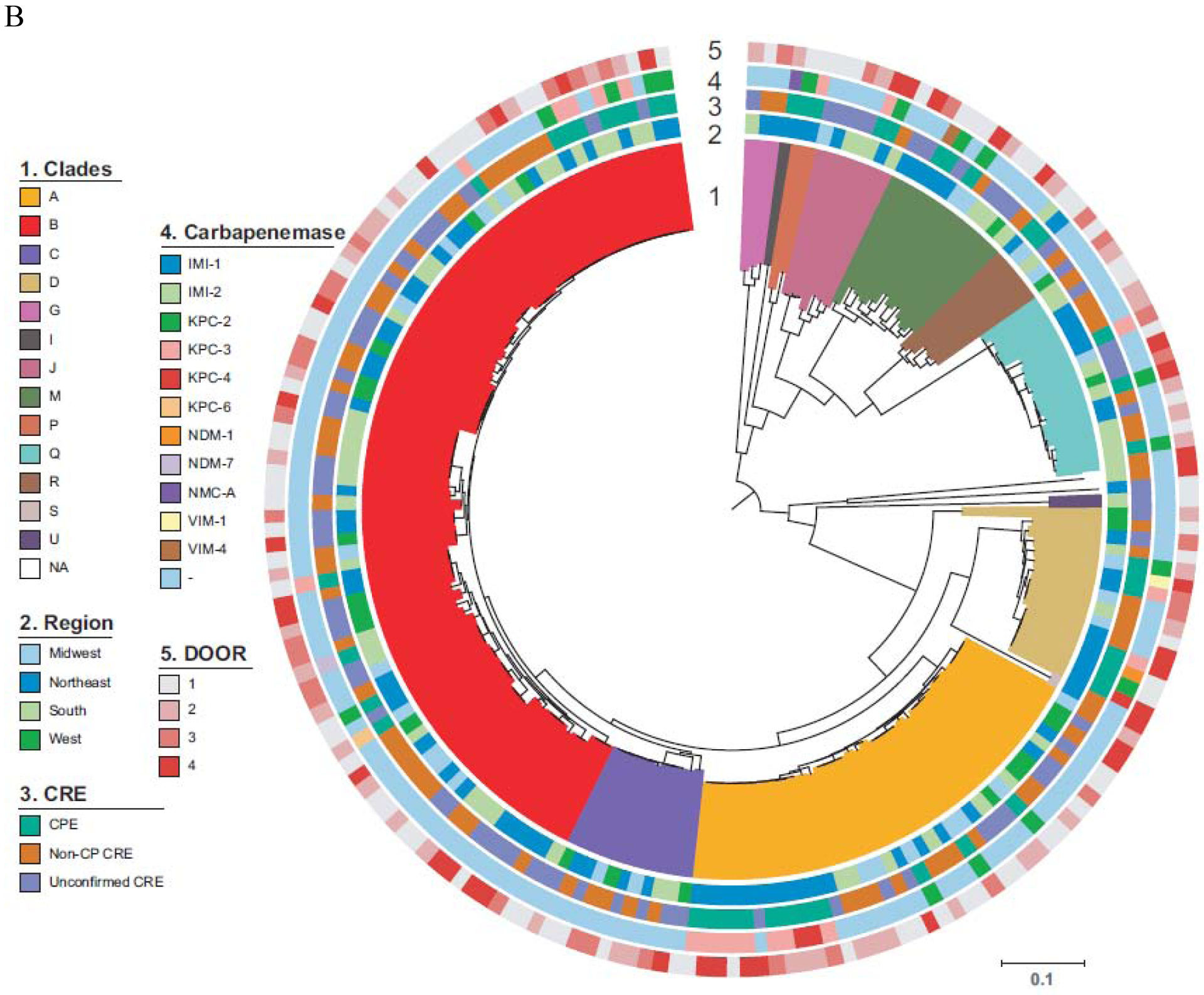
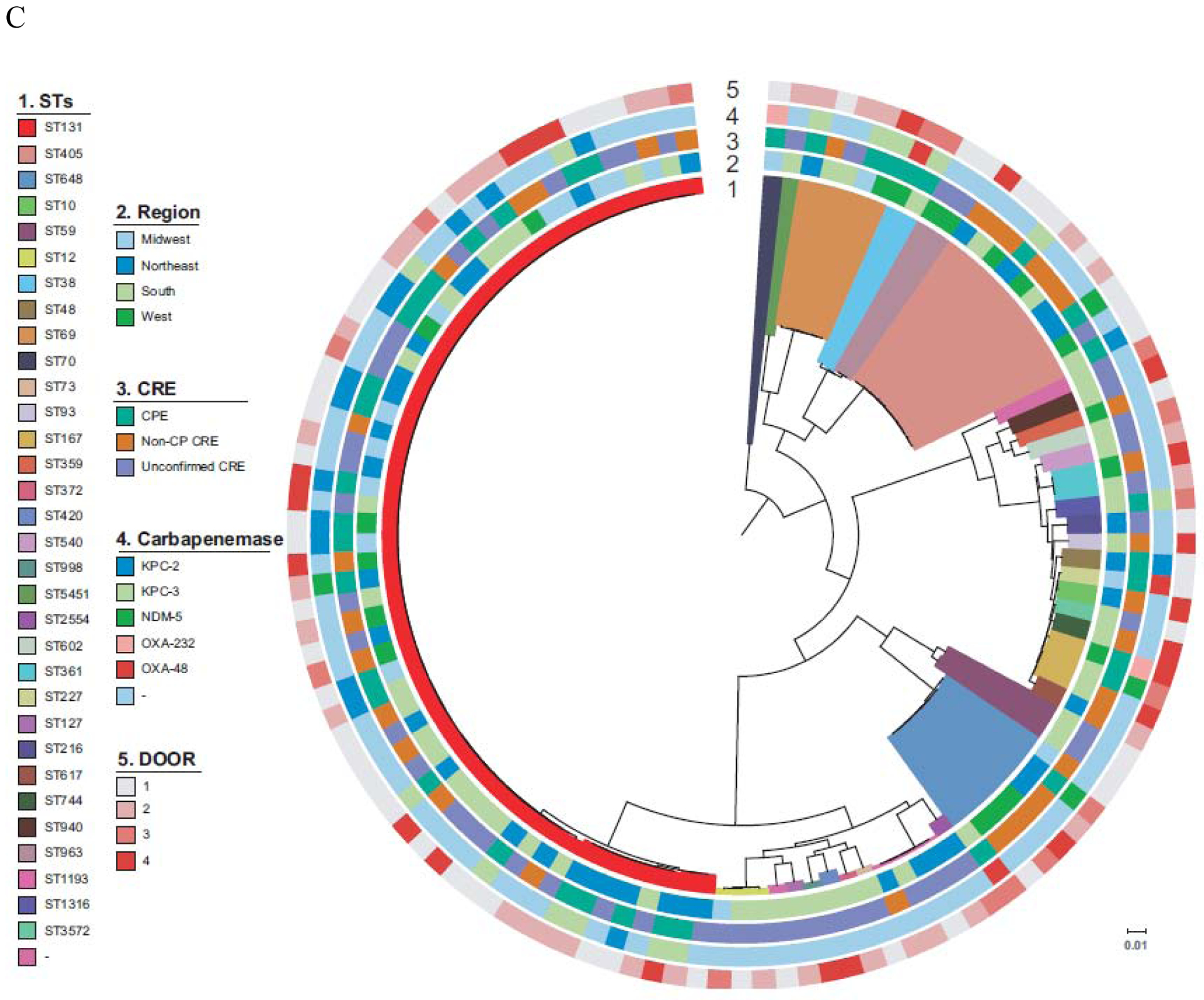
Findings: 1040 patients with unique isolates were included, 449 (43%) with infection and 591 (57%) with colonisation. The CDC-defined CRE admission rate was 57 per 100 000 admissions (95% CI 45-71). Three subsets of CDC-defined CRE were identified: carbapenemase-producing Enterobacterales (618 [59%] of 1040), non-carbapenemase-producing Enterobacterales (194 [19%]), and unconfirmed CRE (228 [22%]; initially reported as CRE, but susceptible to carbapenems in two central laboratories). Klebsiella pneumoniae carbapenemase-producing clonal group 258 K pneumoniae was the most common carbapenemase-producing Enterobacterales. In 449 patients with CDC-defined CRE infections, DOOR outcomes were not significantly different in patients with carbapenemase-producing Enterobacterales, non-carbapenemase-producing Enterobacterales, and unconfirmed CRE. At 30 days 107 (24%, 95% CI 20-28) of these patients had died.
Interpretation: Among patients with CDC-defined CRE, similar outcomes were observed among three subgroups, including the novel unconfirmed CRE group. CDC-defined CRE represent diverse bacteria, whose spread might not respond to interventions directed to carbapenemase-producing Enterobacterales.
Funding: National Institutes of Health.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Carbapenem-resistant Enterobacterales in the USA.Lancet Infect Dis. 2020 Jun;20(6):637-639. doi: 10.1016/S1473-3099(20)30066-9. Epub 2020 Mar 6. Lancet Infect Dis. 2020. PMID: 32151330 No abstract available.
References
-
- World Health Organization. WHO priority pathogens list for R&D of new antibiotics. 2017; http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-n....
-
- Bush K. Carbapenemases: Partners in crime. J Glob Antimicrob Resist 2013; 1(1): 7–16. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 AI100560/AI/NIAID NIH HHS/United States
- R01 AI104895/AI/NIAID NIH HHS/United States
- K24 AI093969/AI/NIAID NIH HHS/United States
- R21 AI143229/AI/NIAID NIH HHS/United States
- I01 BX003741/BX/BLRD VA/United States
- R01 AI072219/AI/NIAID NIH HHS/United States
- R01 AI119446/AI/NIAID NIH HHS/United States
- R01 AI063517/AI/NIAID NIH HHS/United States
- R01 AI143910/AI/NIAID NIH HHS/United States
- R21 AI123747/AI/NIAID NIH HHS/United States
- K24 AI121296/AI/NIAID NIH HHS/United States
- I01 BX001974/BX/BLRD VA/United States
- WT_/Wellcome Trust/United Kingdom
- K08 AI113317/AI/NIAID NIH HHS/United States
- R21 AI114508/AI/NIAID NIH HHS/United States
- R21 AI135522/AI/NIAID NIH HHS/United States
- R21 AI117338/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R01 AI090155/AI/NIAID NIH HHS/United States
- R01 AI134637/AI/NIAID NIH HHS/United States
- R21 AI135250/AI/NIAID NIH HHS/United States
- UM1 AI104681/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
