

Screening strategies to identify sepsis in the prehospital setting: a validation study
- PMID: 32152051
- PMCID: PMC7062432
- DOI: 10.1503/cmaj.190966
Screening strategies to identify sepsis in the prehospital setting: a validation study
Abstract
Background: In the prehospital setting, differentiating patients who have sepsis from those who have infection but no organ dysfunction is important to initiate sepsis treatments appropriately. We aimed to identify which published screening strategies for paramedics to use in identifying patients with sepsis provide the most certainty for prehospital diagnosis.
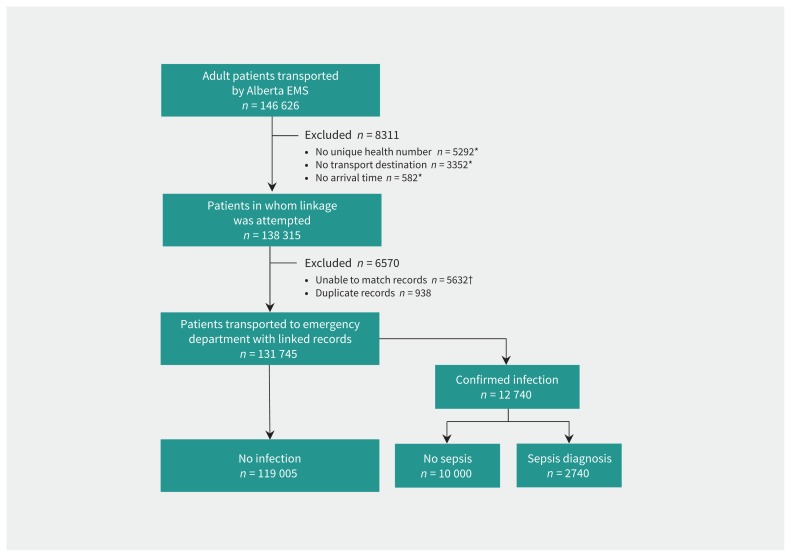
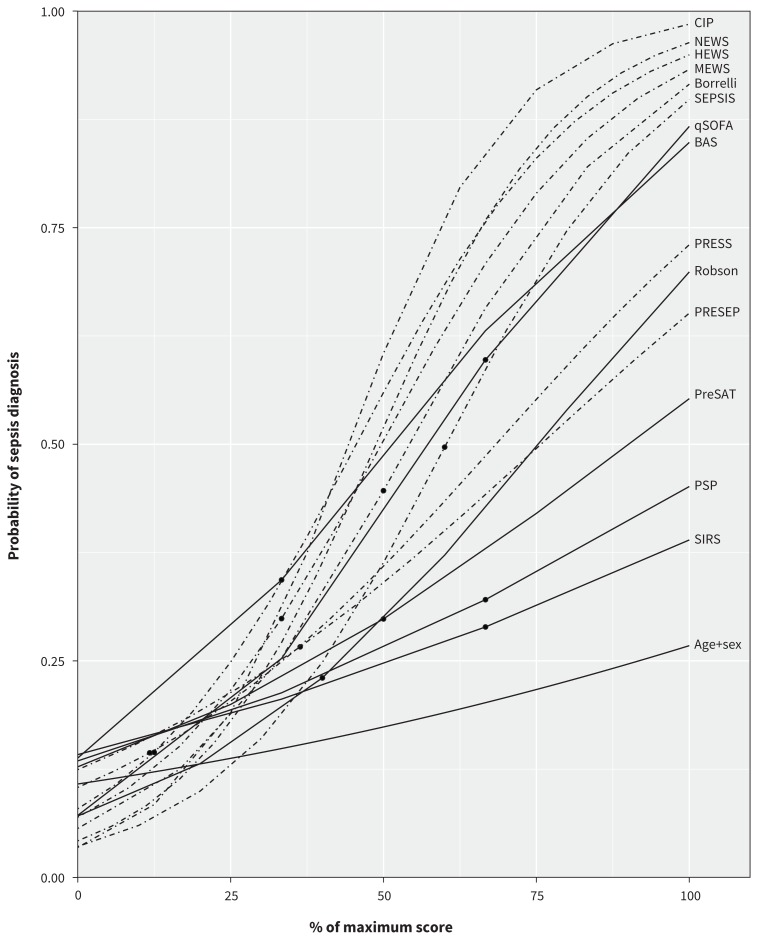
Methods: We identified published strategies for screening by paramedics through a literature search. We then conducted a validation study in Alberta, Canada, from April 2015 to March 2016. For adult patients (≥ 18 yr) who were transferred by ambulance, we linked records to an administrative database and then restricted the search to patients with infection diagnosed in the emergency department. For each patient, the classification from each strategy was determined and compared with the diagnosis recorded in the emergency department. For all strategies that generated numeric scores, we constructed diagnostic prediction models to estimate the probability of sepsis being diagnosed in the emergency department.
Results: We identified 21 unique prehospital screening strategies, 14 of which had numeric scores. We linked a total of 131 745 eligible patients to hospital databases. No single strategy had both high sensitivity (overall range 0.02-0.85) and high specificity (overall range 0.38-0.99) for classifying sepsis. However, the Critical Illness Prediction (CIP) score, the National Early Warning Score (NEWS) and the Quick Sepsis-Related Organ Failure Assessment (qSOFA) score predicted a low to high probability of a sepsis diagnosis at different scores. The qSOFA identified patients with a 7% (lowest score) to 87% (highest score) probability of sepsis diagnosis.
Interpretation: The CIP, NEWS and qSOFA scores are tools with good predictive ability for sepsis diagnosis in the prehospital setting. The qSOFA score is simple to calculate and may be useful to paramedics in screening patients with possible sepsis.
© 2020 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Sheldon Cheskes has received investigator-initiated grant funding from Zoll Medical for several research programs (AED on the Fly, Community Responder Program for Out-of-Hospital Cardiac Arrest and Measuring Ventilation During Out-of-Hospital Cardiac Arrest). He also sits on the advisory board of Drone Delivery Canada. Damon Scales holds operating grants from the Canadian Institutes of Health Research. No other competing interests were declared.
Figures
Similar articles
-
Classification versus Prediction of Mortality Risk using the SIRS and qSOFA Scores in Patients with Infection Transported by Paramedics.Prehosp Emerg Care. 2020 Mar-Apr;24(2):282-289. doi: 10.1080/10903127.2019.1624901. Epub 2019 Jun 19. Prehosp Emerg Care. 2020. PMID: 31140890
-
Superior performance of National Early Warning Score compared with quick Sepsis-related Organ Failure Assessment Score in predicting adverse outcomes: a retrospective observational study of patients in the prehospital setting.Eur J Emerg Med. 2019 Dec;26(6):433-439. doi: 10.1097/MEJ.0000000000000589. Eur J Emerg Med. 2019. PMID: 30585862
-
qSOFA Has Poor Sensitivity for Prehospital Identification of Severe Sepsis and Septic Shock.Prehosp Emerg Care. 2017 Jul-Aug;21(4):489-497. doi: 10.1080/10903127.2016.1274348. Epub 2017 Jan 25. Prehosp Emerg Care. 2017. PMID: 28121217
-
Early Recognition of Sepsis in Prehospital Settings: A Review of Screening Tools and Practices.Adv Emerg Nurs J. 2025 Apr-Jun 01;47(2):152-167. doi: 10.1097/TME.0000000000000561. Epub 2025 Apr 1. Adv Emerg Nurs J. 2025. PMID: 40168615 Review.
-
Evidence for Use of Validated Sepsis Screening Tools in the Prehospital Population: A Scoping Review.Prehosp Emerg Care. 2024;28(3):485-493. doi: 10.1080/10903127.2023.2224862. Epub 2023 Jul 6. Prehosp Emerg Care. 2024. PMID: 37327065
Cited by
-
Prehospital early warning scores for adults with suspected sepsis: retrospective diagnostic cohort study.Emerg Med J. 2023 Nov;40(11):768-776. doi: 10.1136/emermed-2023-213315. Epub 2023 Sep 6. Emerg Med J. 2023. PMID: 37673643 Free PMC article.
-
Performance Evaluation of Prehospital Sepsis Prediction Models.Crit Care Med. 2025 Apr 1;53(4):e973-e978. doi: 10.1097/CCM.0000000000006586. Epub 2025 Feb 12. Crit Care Med. 2025. PMID: 39937065
-
Diagnostic Delays in Sepsis: Lessons Learned From a Retrospective Study of Canadian Medico-Legal Claims.Crit Care Explor. 2023 Feb 1;5(2):e0841. doi: 10.1097/CCE.0000000000000841. eCollection 2023 Feb. Crit Care Explor. 2023. PMID: 36751515 Free PMC article.
-
Is Prehospital Assessment of qSOFA Parameters Associated with Earlier Targeted Sepsis Therapy? A Retrospective Cohort Study.J Clin Med. 2022 Jun 17;11(12):3501. doi: 10.3390/jcm11123501. J Clin Med. 2022. PMID: 35743570 Free PMC article.
-
Sepsis and case fatality rates and associations with deprivation, ethnicity, and clinical characteristics: population-based case-control study with linked primary care and hospital data in England.Infection. 2024 Aug;52(4):1469-1479. doi: 10.1007/s15010-024-02235-8. Epub 2024 Apr 16. Infection. 2024. PMID: 38627354 Free PMC article.
References
-
- Executive Board, 140th session. Improving the prevention, diagnosis and clinical management of sepsis. Report by the Secretariat. Geneva: World Health Organization; 2017.
-
- Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med 2017;45:486–552. - PubMed
-
- Lane D, Ichelson RI, Drennan IR, et al. Prehospital management and identification of sepsis by emergency medical services: a systematic review. Emerg Med J 2016;33:408–13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous