

Complications and discomfort after research bronchoscopy in the MicroCOPD study
- PMID: 32152177
- PMCID: PMC7064136
- DOI: 10.1136/bmjresp-2019-000449
Complications and discomfort after research bronchoscopy in the MicroCOPD study
Abstract
Background: Data on discomfort and complications from research bronchoscopy in chronic obstructive pulmonary disease (COPD) and asthma is limited. We present complications and discomfort occurring within a week after bronchoscopy, and investigate personal and procedural risk factors.
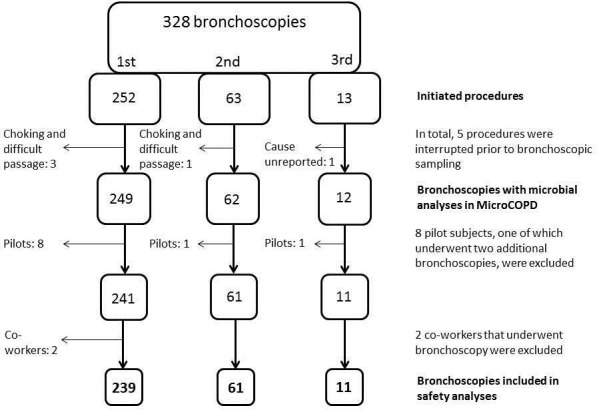
Methods: 239 subjects with COPD, asthma or without lung disease underwent research bronchoscopies as part of a microbiome study of the lower airways (the MicroCOPD study). Bronchoscopy was done in the supine position with oral scope insertion with the option of light conscious alfentanil sedation. Sampling consisted of protected specimen brushes, bronchoalveolar lavage, small volume lavage and for some, endobronchial biopsies. Bleeding, desaturation, cough, haemodynamic changes, dyspnoea and other events that required an unplanned intervention or early termination of bronchoscopy were prospectively recorded. Follow-up consisted of a telephone interview where subjects rated discomfort and answered questions about fever sensation and respiratory symptoms in the week following bronchoscopy.
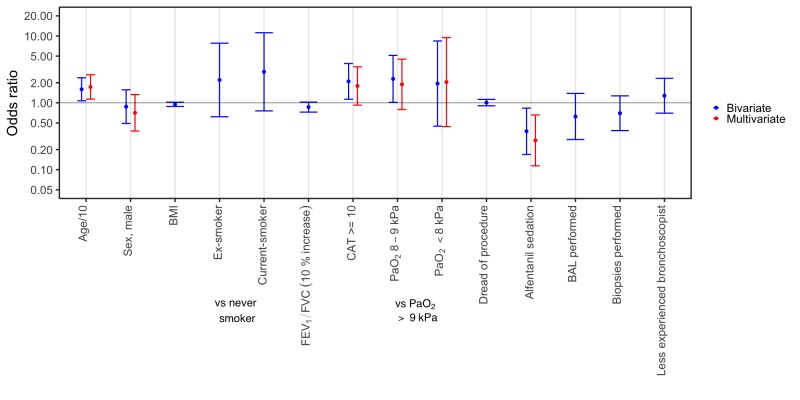
Results: An unplanned intervention or early termination of bronchoscopy was required in 25.9% of bronchoscopies. Three subjects (1.3%) experienced potentially severe complications, of which all recovered without sequelae. COPD subjects experienced more dyspnoea than controls. Sedation and lower age was associated with less unplanned intervention or premature termination. About half of the subjects (47.7%) reported fever. Discomfort was associated with postprocedural fever, dread of bronchoscopy, higher score on the COPD Assessment Test and never-smoking. In subjects undergoing more than one bronchoscopy, the first bronchoscopy was often predictive for complications and postprocedural fever in the repeated bronchoscopy.
Conclusion: Research bronchoscopies were not associated with more complications or discomfort in COPD subjects. 47.7% experienced postbronchoscopy fever sensation, which was associated with discomfort.
Keywords: COPD epidemiology; bronchoscopy.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: EOL, EMHM, EN, KSK, ØS and PSB declare no competing interests. TMLE has for the last three years received lecture fees from Boehringer Ingelheim, Roche and Astra Zeneca. GRH has for the last three years received lecture fees from Novartis and Boehringer Ingelheim. RN reports grants from GlaxoSmithKline, during the conduct of the study; grants from Boehringer Ingelheim, grants and personal fees from AstraZeneca, grants from Novartis, personal fees from GlaxoSmithKline, outside the submitted work. SL has for the last three years received lecture fees from Philips, Novartis and Astra Zeneca, and advisory board fees (paid to employer) from Novartis and Astra Zeneca, all outside the submitted work.
Figures
References
-
- Grendelmeier P, Kurer G, Pflimlin E, et al. Feasibility and safety of propofol sedation in flexible bronchoscopy. Swiss Med Wkly 2011;141:w13248. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical