

Severity of oro-dental anomalies in Loeys-Dietz syndrome segregates by gene mutation
- PMID: 32152251
- PMCID: PMC7525783
- DOI: 10.1136/jmedgenet-2019-106678
Severity of oro-dental anomalies in Loeys-Dietz syndrome segregates by gene mutation
Abstract
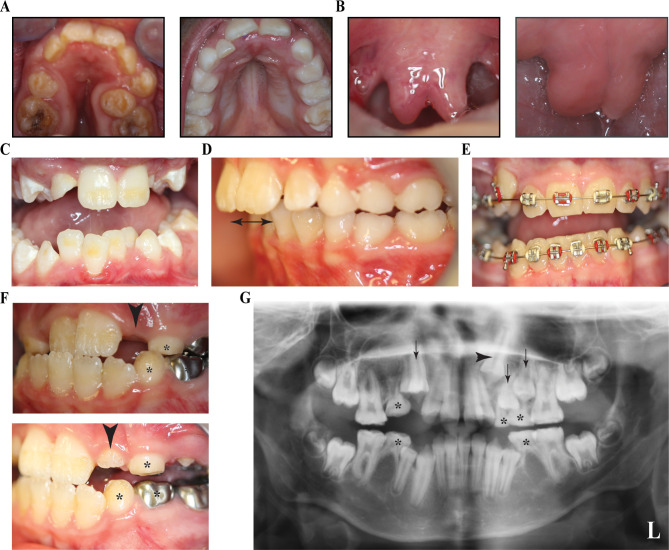
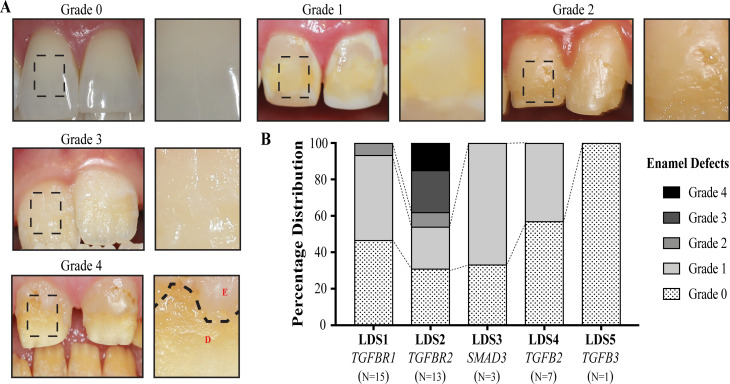
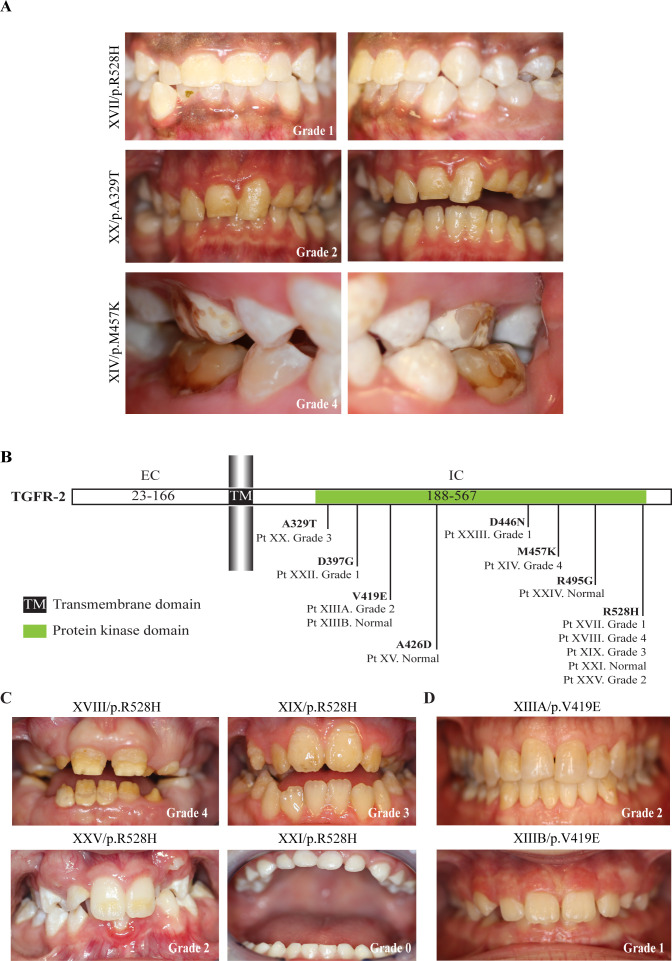
Background Loeys-Dietz syndrome (LDS), an autosomal dominant rare connective tissue disorder, has multisystemic manifestations, characterised by vascular tortuosity, aneurysms and craniofacial manifestations. Based on the associated gene mutations along the transforming growth factor-beta (TGF-β) pathway, LDS is presently classified into six subtypes. Methods We present the oro-dental features of a cohort of 40 patients with LDS from five subtypes. Results The most common oro-dental manifestations were the presence of a high-arched and narrow palate, and enamel defects. Other common characteristics included bifid uvula, submucous cleft palate, malocclusion, dental crowding and delayed eruption of permanent teeth. Both deciduous and permanent teeth had enamel defects in some individuals. We established a grading system to measure the severity of enamel defects, and we determined that the severity of the enamel anomalies in LDS is subtype-dependent. In specific, patients with TGF-β receptor II mutations (LDS2) presented with the most severe enamel defects, followed by patients with TGF-β receptor I mutations (LDS1). LDS2 patients had higher frequency of oro-dental deformities in general. Across all five subtypes, as well as within each subtype, enamel defects exhibited incomplete penetrance and variable expression, which is not associated with the location of the gene mutations. Conclusion This study describes, in detail, the oro-dental manifestations in a cohort of LDS, and we conclude that LDS2 has the most severely affected phenotype. This extensive characterisation, as well as some identified distinguishing features can significantly aid dental and medical care providers in the diagnosis and clinical management of patients with this rare connective tissue disorder.
Keywords: connective tissue disease; diagnosis; genetics; getting research into practice.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Distinctive Amelogenesis Imperfecta in Loeys-Dietz Syndrome Type II.J Dent Res. 2025 Jul;104(8):840-850. doi: 10.1177/00220345251326094. Epub 2025 Apr 22. J Dent Res. 2025. PMID: 40261094
-
Genotypic Categorization of Loeys-Dietz Syndrome Based on 24 Novel Families and Literature Data.Genes (Basel). 2019 Sep 28;10(10):764. doi: 10.3390/genes10100764. Genes (Basel). 2019. PMID: 31569402 Free PMC article. Review.
-
Clinical diagnosis of Larsen syndrome, Stickler syndrome and Loeys-Dietz syndrome in a 19-year old male: a case report.BMC Med Genet. 2018 Aug 31;19(1):155. doi: 10.1186/s12881-018-0671-0. BMC Med Genet. 2018. PMID: 30170566 Free PMC article.
-
Dental Considerations in Patients with Loeys-Dietz Syndrome: A Review of the Literature and Case Report.J Clin Pediatr Dent. 2021 Jul 1;45(3):193-198. doi: 10.17796/1053-4625-45.3.8. J Clin Pediatr Dent. 2021. PMID: 34192753 Review.
-
Loeys-Dietz syndrome type I and type II: clinical findings and novel mutations in two Italian patients.Orphanet J Rare Dis. 2009 Nov 2;4:24. doi: 10.1186/1750-1172-4-24. Orphanet J Rare Dis. 2009. PMID: 19883511 Free PMC article.
Cited by
-
The peroxisomal disorder spectrum and Heimler syndrome: Deep phenotyping and review of the literature.Am J Med Genet C Semin Med Genet. 2020 Sep;184(3):618-630. doi: 10.1002/ajmg.c.31823. Epub 2020 Aug 31. Am J Med Genet C Semin Med Genet. 2020. PMID: 32866347 Free PMC article.
-
Genotype-Phenotype Correlation Insights Through Molecular Modeling Analysis in a Patient with Loeys-Dietz Syndrome.Genes (Basel). 2025 Mar 21;16(4):357. doi: 10.3390/genes16040357. Genes (Basel). 2025. PMID: 40282317 Free PMC article.
-
Loeys-Dietz and Shprintzen-Goldberg syndromes: analysis of TGF-β-opathies with craniofacial manifestations using an innovative multimodality method.J Med Genet. 2022 Oct;59(10):938-946. doi: 10.1136/jmedgenet-2021-107695. Epub 2021 Dec 16. J Med Genet. 2022. PMID: 34916229 Free PMC article.
-
Craniofacial disorders and dysplasias: Molecular, clinical, and management perspectives.Bone Rep. 2024 Mar 1;20:101747. doi: 10.1016/j.bonr.2024.101747. eCollection 2024 Mar. Bone Rep. 2024. PMID: 38566929 Free PMC article. Review.
-
Impaired Tertiary Dentin Secretion after Shallow Injury in Tgfbr2-Deficient Dental Pulp Cells Is Rescued by Extended CGRP Signaling.Int J Mol Sci. 2024 Jun 21;25(13):6847. doi: 10.3390/ijms25136847. Int J Mol Sci. 2024. PMID: 38999956 Free PMC article.
References
-
- National Institutes of Health RDD Available: https://rarediseases.info.nih.gov/diseases/diseases-by-category/23/mouth...
-
- Bloch-Zupan A, Sedano HO, Scully C. 1 - Odontogenesis, anomalies and genetics : Bloch-Zupan A, Sedano HO, Scully C, Dento/Oro/Craniofacial anomalies and genetics. London: Elsevier, 2012: 1–8.
-
- Gorlin RJ, Cohen Jr MM, Hennekam RC. Syndromes of the head and neck. Oxford university press, 2001.
-
- Loeys BL, Chen J, Neptune ER, Judge DP, Podowski M, Holm T, Meyers J, Leitch CC, Katsanis N, Sharifi N, Xu FL, Myers LA, Spevak PJ, Cameron DE, De Backer J, Hellemans J, Chen Y, Davis EC, Webb CL, Kress W, Coucke P, Rifkin DB, De Paepe AM, Dietz HC. A syndrome of altered cardiovascular, craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat Genet 2005;37:275–81. 10.1038/ng1511 - DOI - PubMed
-
- Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H, De Backer JF, Oswald GL, Symoens S, Manouvrier S, Roberts AE, Faravelli F, Greco MA, Pyeritz RE, Milewicz DM, Coucke PJ, Cameron DE, Braverman AC, Byers PH, De Paepe AM, Dietz HC. Aneurysm syndromes caused by mutations in the TGF-beta receptor. N Engl J Med 2006;355:788–98. 10.1056/NEJMoa055695 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical