

Plasma Cell Myeloma with an Aggressive Clinical Course and Anaplastic Morphology in a 22-Year-Old Patient: A Case Report and Review of Literature
- PMID: 32152261
- PMCID: PMC7081950
- DOI: 10.12659/AJCR.920489
Plasma Cell Myeloma with an Aggressive Clinical Course and Anaplastic Morphology in a 22-Year-Old Patient: A Case Report and Review of Literature
Abstract
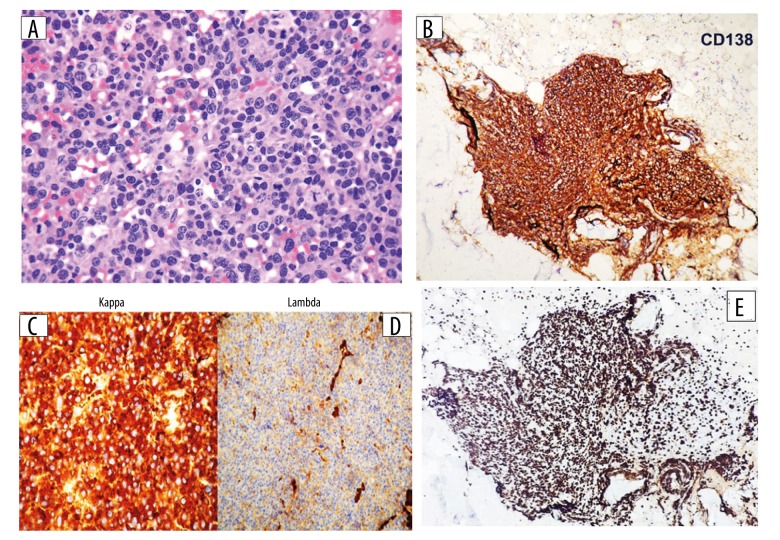
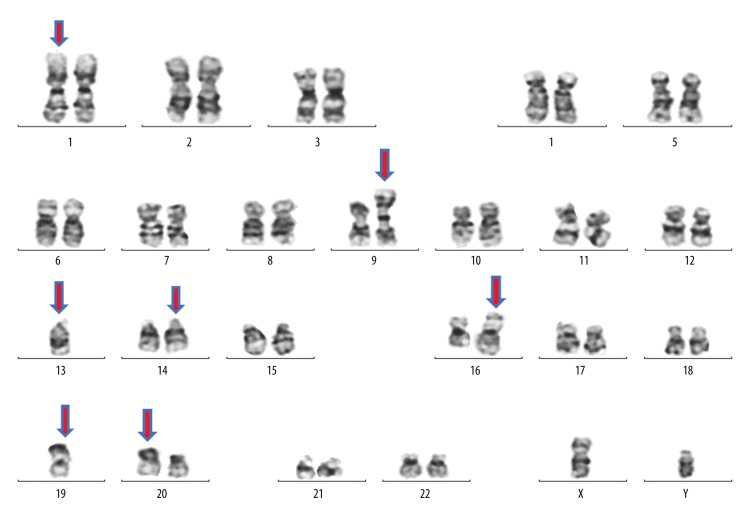
BACKGROUND Plasma cell myeloma is a neoplastic plasma cell disorder that usually presents after the fifth decade of life; it is rarely described in younger population especially under 30 years of age. However, there are conflicting reports in the literature about the clinical behavior and overall survival in younger age groups. In approximately 2% of plasma cell myeloma, the morphology of the neoplastic cells is highly pleomorphic, quite anaplastic, and may resemble metastatic tumor cells. While this poses a challenge for morphological interpretation during diagnosis, it has been demonstrated that bone marrow morphologic features (including diffuse sheet growth pattern, immature cell morphology and high mitotic index) significantly correlates with high risk disease. Moreover, there is limited description available about the morphology of the neoplastic cells when correlating the age at presentation with the clinical outcome/biological behavior; hence, the need to report and collect such cases. CASE REPORT We report a case of plasma cell myeloma in a 22-year-old male who presented with non-specific clinical features and posed a diagnostic challenge during clinical, radiological, and laboratory examination. The pathology specimens showed anaplastic morphology. Unfortunately, after diagnosis, despite treatment with brotezomib, his disease had an aggressive clinical course and he passed away 4 months after diagnosis. CONCLUSIONS Although plasma cell myeloma is rare in patients younger than 30 years, it must be considered in the differential diagnosis and investigated properly especially in patients with clinical suspicion of a metastatic non-hematological tumor. The anaplastic variant in a young patient is a diagnostic challenge and is associated with bizarre morphology, aggressive presentation, adverse cytogenetics, resistance to chemotherapy, and poor, short-term, survival.
Conflict of interest statement
None.
Figures
References
-
- Michels TC, Petersen KE. Multiple myeloma: Diagnosis and treatment. Am Fam Physician. 2017;95(6):373–83. - PubMed
-
- Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21–33. - PubMed
-
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–48. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
