

The tubular hypothesis of nephron filtration and diabetic kidney disease
- PMID: 32152499
- PMCID: PMC7242158
- DOI: 10.1038/s41581-020-0256-y
The tubular hypothesis of nephron filtration and diabetic kidney disease
Abstract
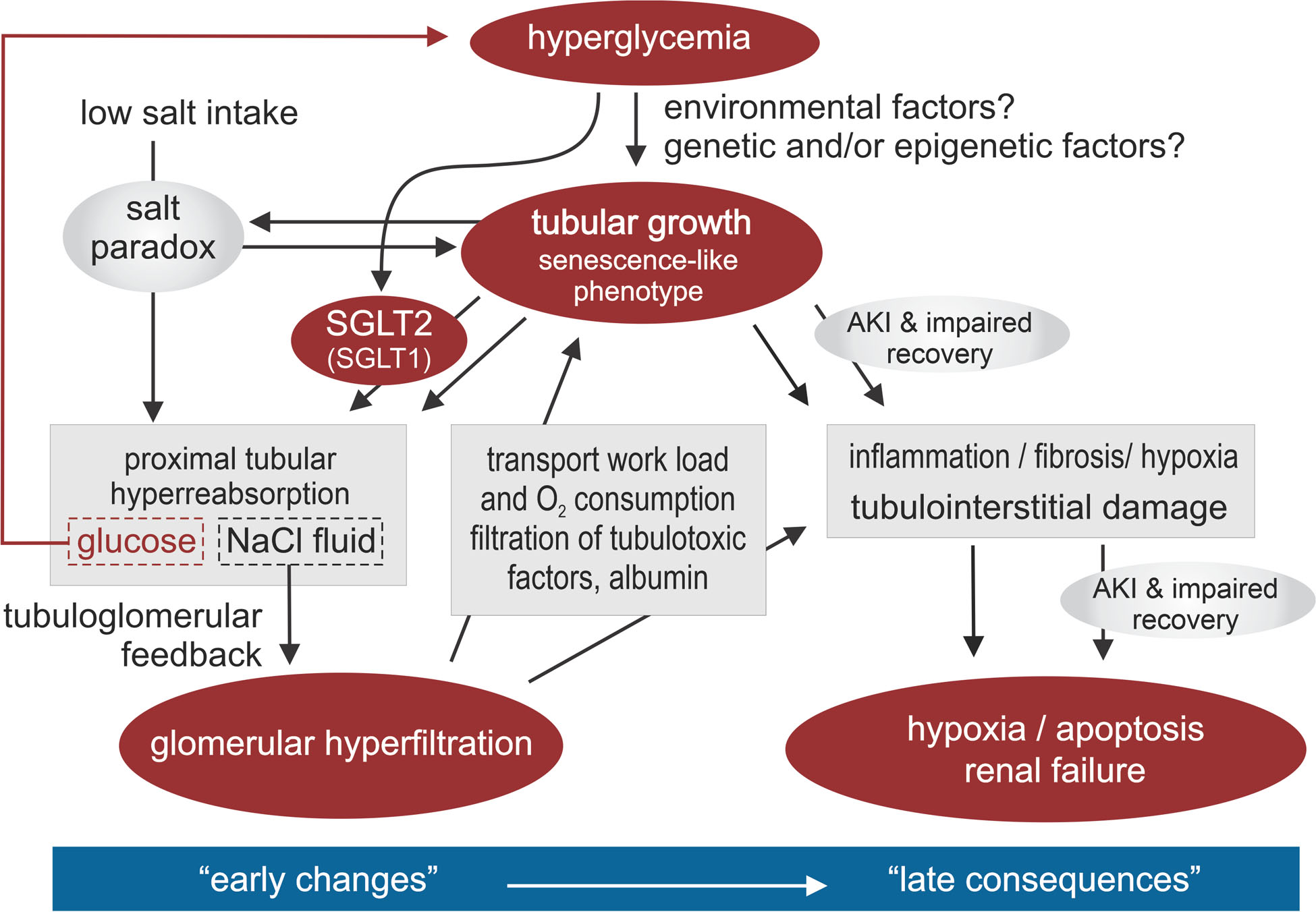
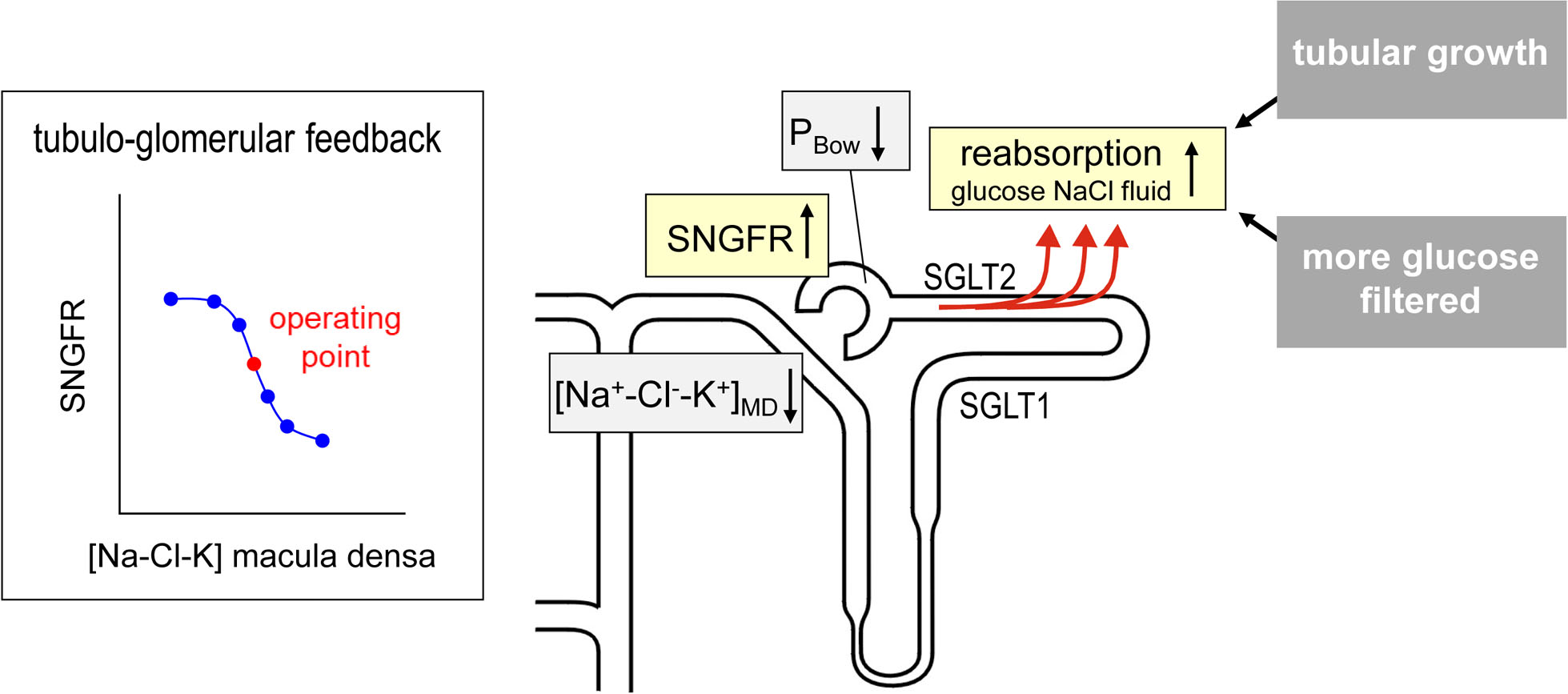
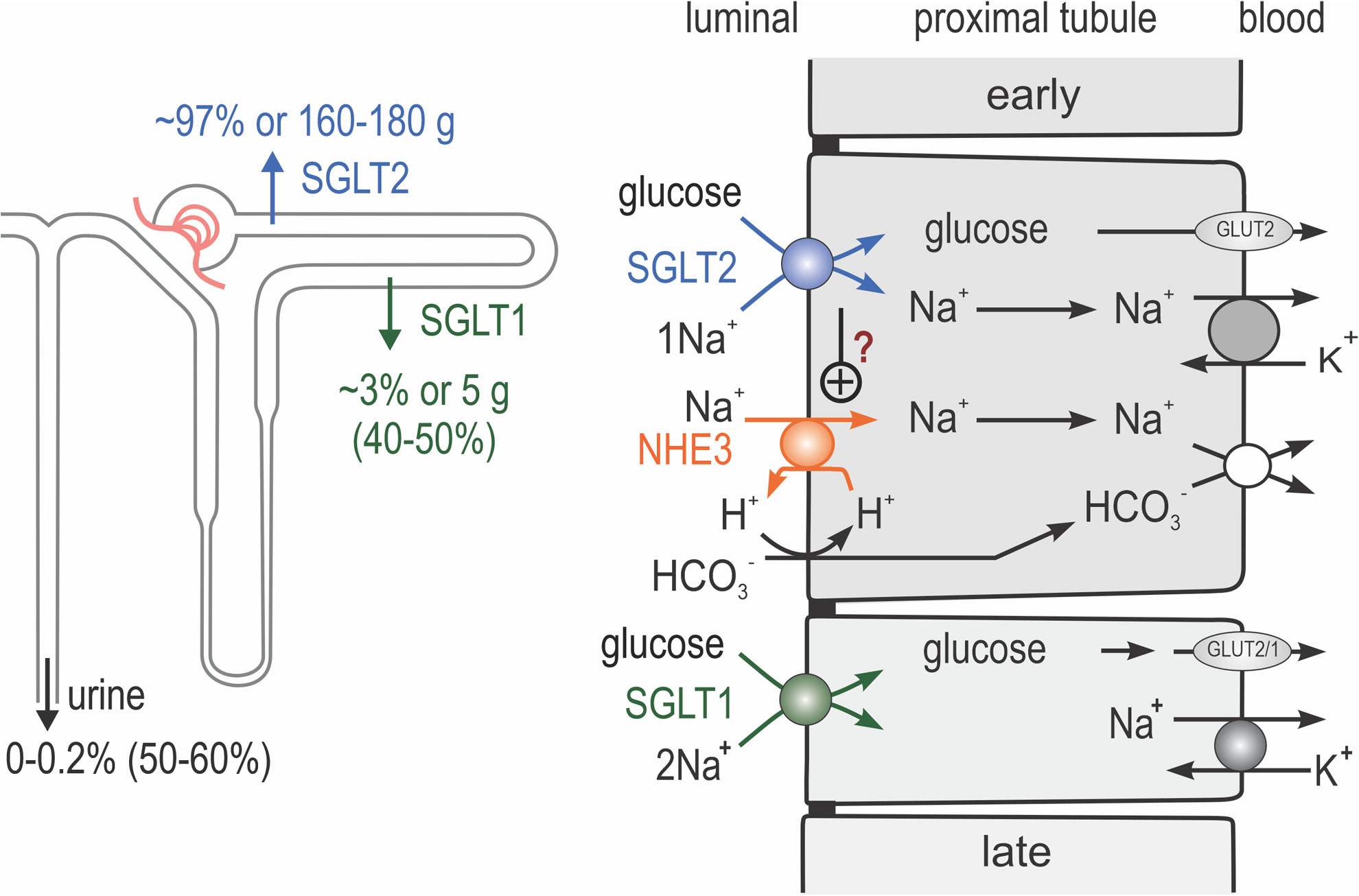
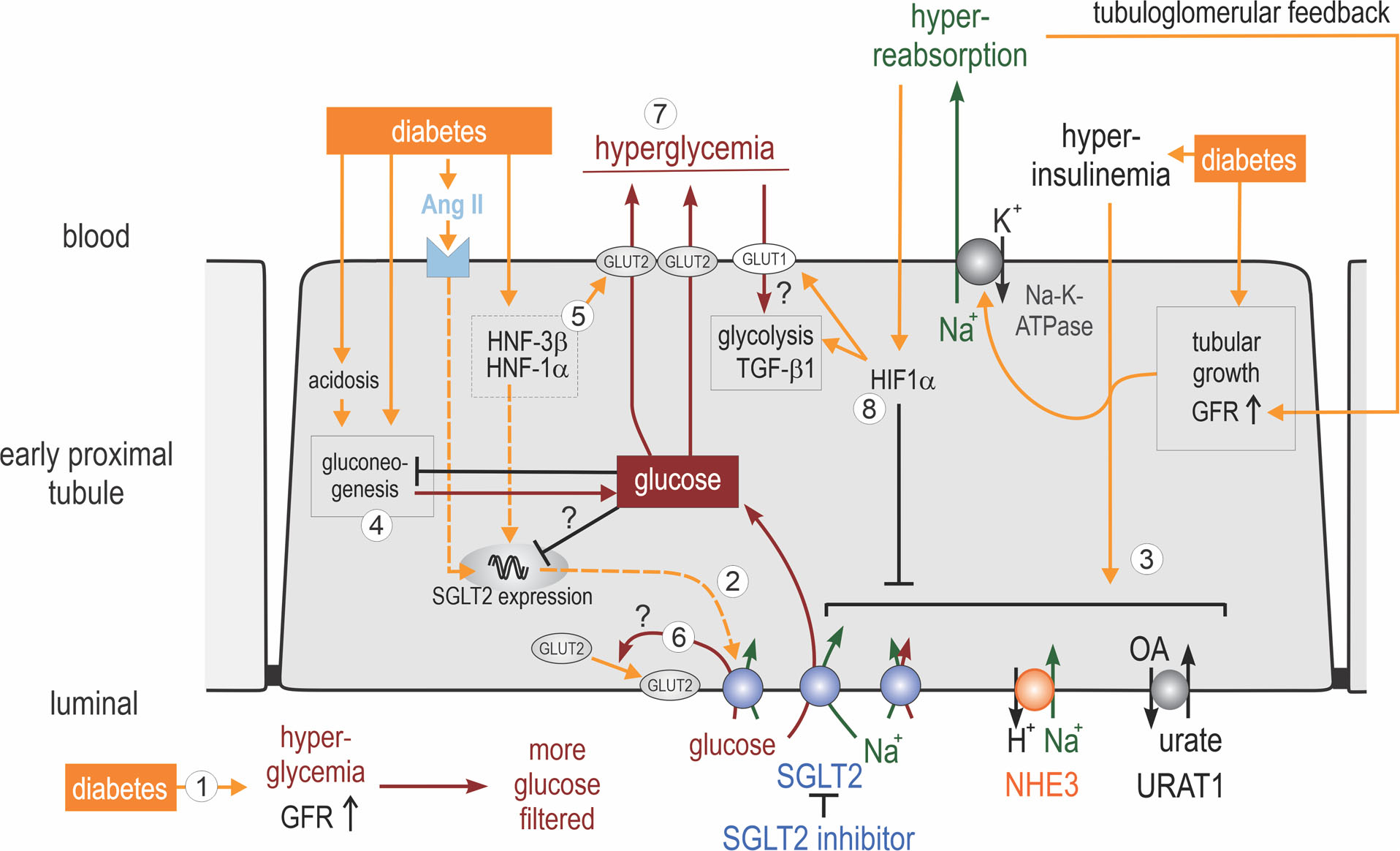
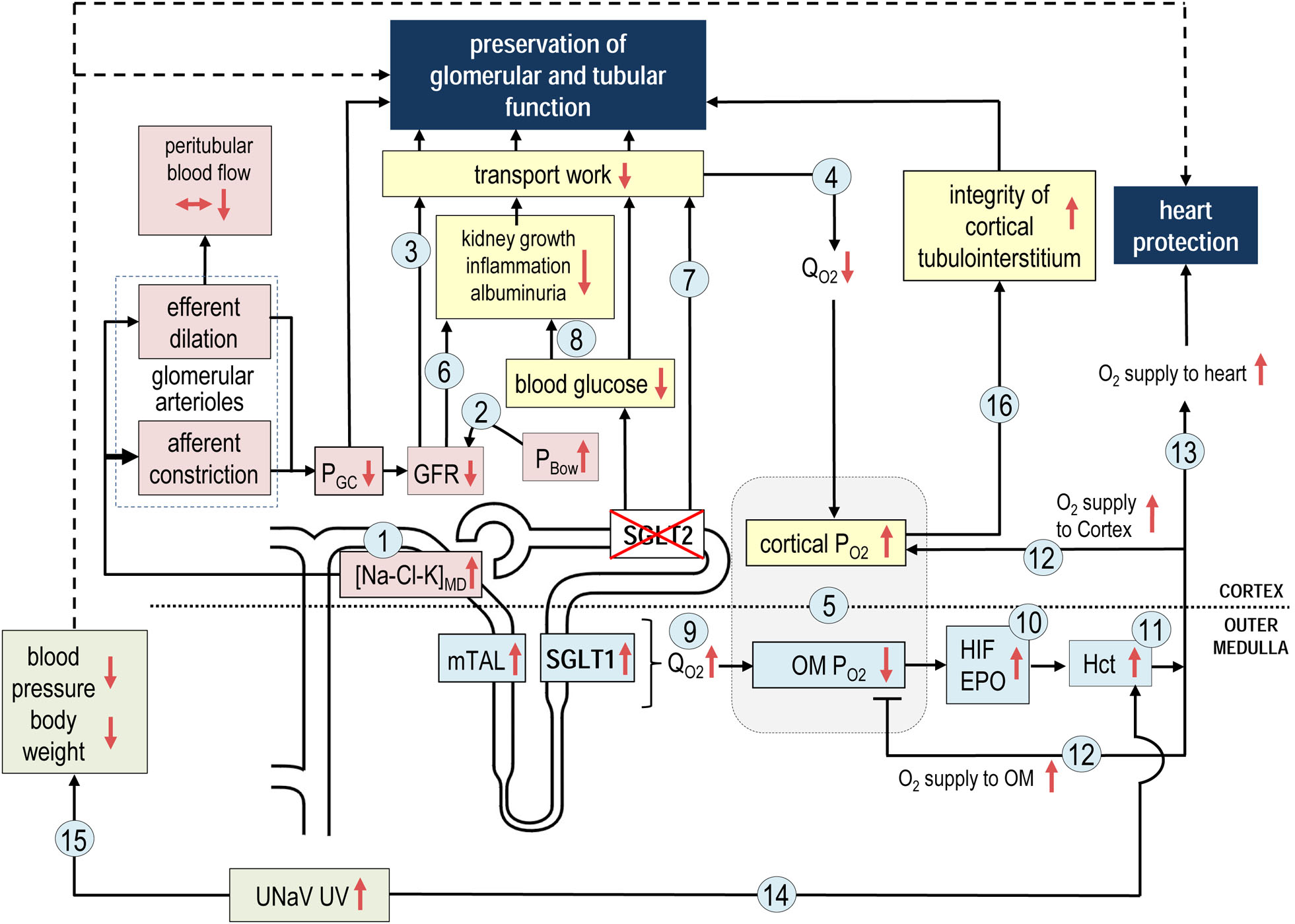
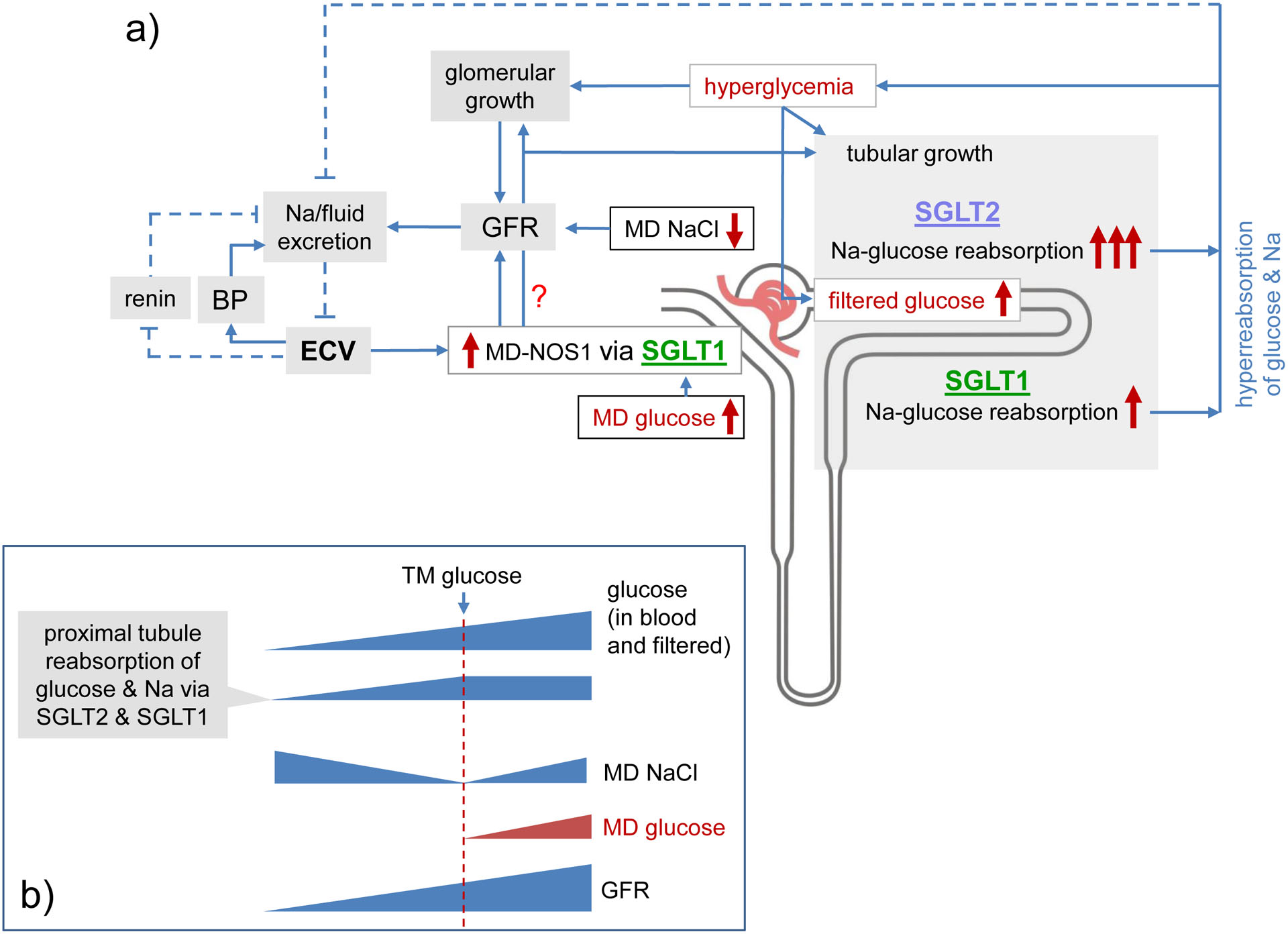
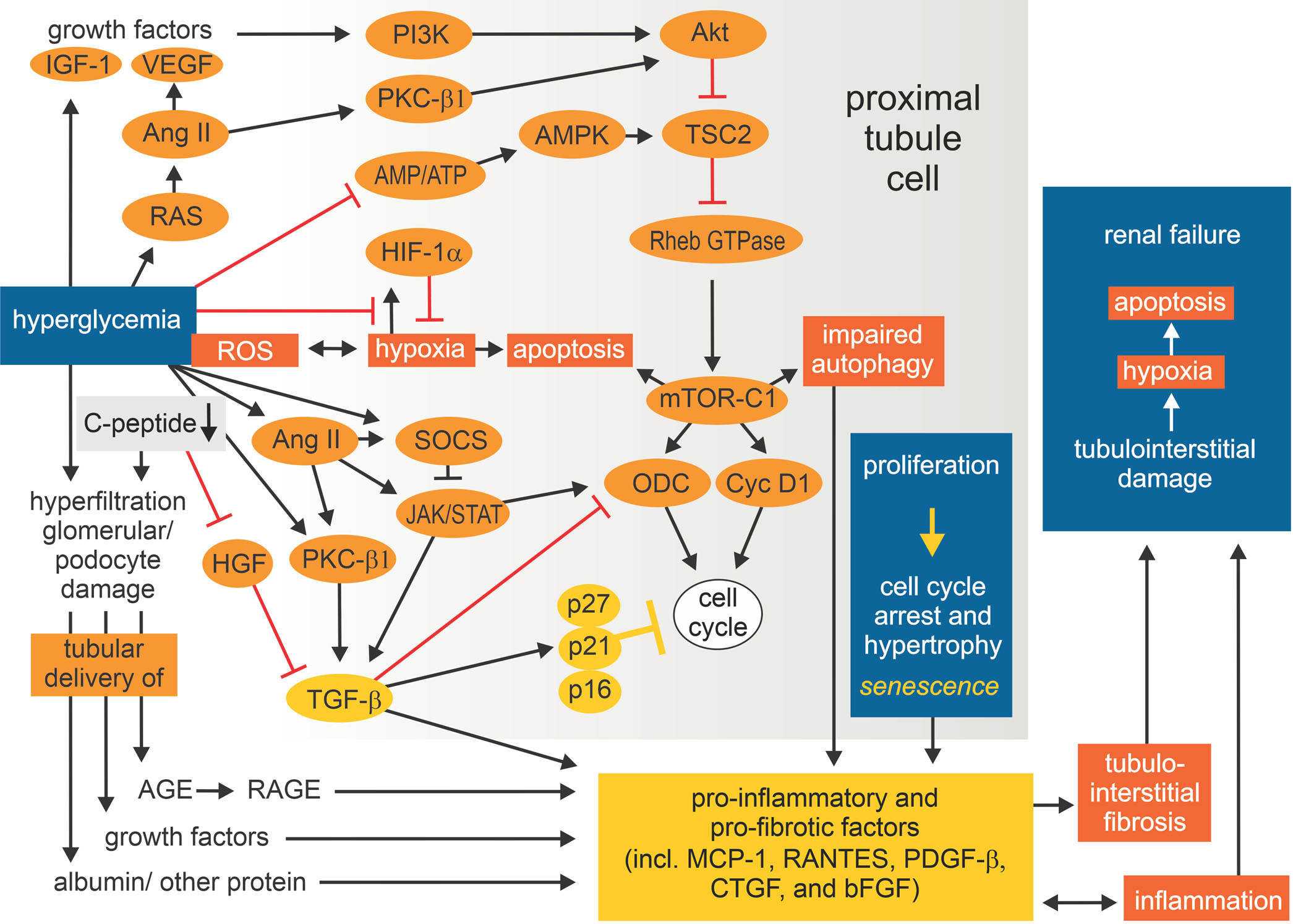
Kidney size and glomerular filtration rate (GFR) often increase with the onset of diabetes, and elevated GFR is a risk factor for the development of diabetic kidney disease. Hyperfiltration mainly occurs in response to signals passed from the tubule to the glomerulus: high levels of glucose in the glomerular filtrate drive increased reabsorption of glucose and sodium by the sodium-glucose cotransporters SGLT2 and SGLT1 in the proximal tubule. Passive reabsorption of chloride and water also increases. The overall capacity for proximal reabsorption is augmented by growth of the proximal tubule, which (alongside sodium-glucose cotransport) further limits urinary glucose loss. Hyperreabsorption of sodium and chloride induces tubuloglomerular feedback from the macula densa to increase GFR. In addition, sodium-glucose cotransport by SGLT1 on macula densa cells triggers the production of nitric oxide, which also contributes to glomerular hyperfiltration. Although hyperfiltration restores sodium and chloride excretion it imposes added physical stress on the filtration barrier and increases the oxygen demand to drive reabsorption. Tubular growth is associated with the development of a senescence-like molecular signature that sets the stage for inflammation and fibrosis. SGLT2 inhibitors attenuate the proximal reabsorption of sodium and glucose, normalize tubuloglomerular feedback signals and mitigate hyperfiltration. This tubule-centred model of diabetic kidney physiology predicts the salutary effect of SGLT2 inhibitors on hard renal outcomes, as shown in large-scale clinical trials.
Conflict of interest statement
Competing interests
V.V. declares that he has served as a consultant and received honoraria from Astra-Zeneca, Bayer, Boehringer Ingelheim, Janssen Pharmaceutical, Eli Lilly, Merck and Retrophin, and has received grant support for investigator-initiated research from Astra-Zeneca, Bayer, Boehringer Ingelheim, Fresenius and Janssen. S.C.T. declares that he has received grant support for investigator-initiated research from Merck.
Figures
References
-
- United States Renal Data System. 2015 Annual Data Report: Epidemiology of kidney disease in the United States, Bethesda, MD. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2015, https://www.usrds.org/2015/view/ (2015).
-
- Jha V et al. Chronic kidney disease: global dimension and perspectives. Lancet 382, 260–272 (2013). - PubMed
-
- Papademetriou V et al. Chronic kidney disease and intensive glycemic control increase cardiovascular risk in patients with type 2 diabetes. Kidney Int 87, 649–659 (2015). - PubMed
-
- Lanting LC, Joung IM, Mackenbach JP, Lamberts SW & Bootsma AH Ethnic differences in mortality, end-stage complications, and quality of care among diabetic patients: a review. Diabetes Care 28, 2280–2288 (2005). - PubMed
