

Longitudinal evaluation of peripheral nerve sheath tumors in neurofibromatosis type 1: growth analysis of plexiform neurofibromas and distinct nodular lesions
- PMID: 32152628
- PMCID: PMC7523449
- DOI: 10.1093/neuonc/noaa053
Longitudinal evaluation of peripheral nerve sheath tumors in neurofibromatosis type 1: growth analysis of plexiform neurofibromas and distinct nodular lesions
Abstract
Background: Understanding the natural history of non-malignant peripheral nerve sheath tumors (PNSTs) in neurofibromatosis type 1 (NF1) is critical to optimal clinical care and the development of meaningful clinical trials.
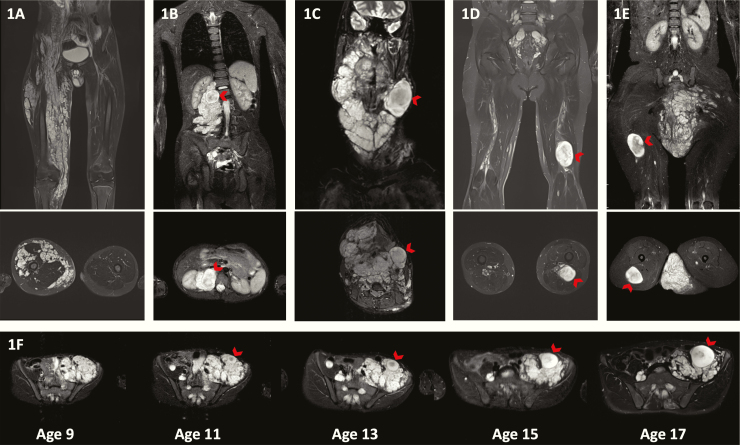
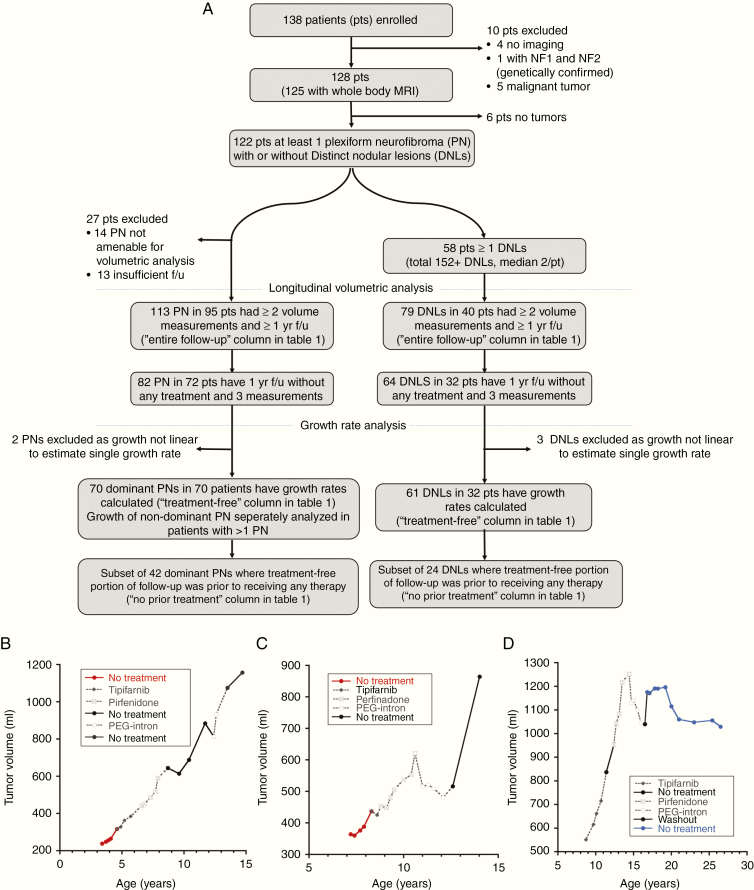
Methods: We longitudinally analyzed growth of plexiform neurofibromas (PNs) and of PNSTs with distinct nodular appearance (distinct nodular lesions [DNLs]) using volumetric MRI analysis in patients enrolled on a natural history study (NCT00924196).
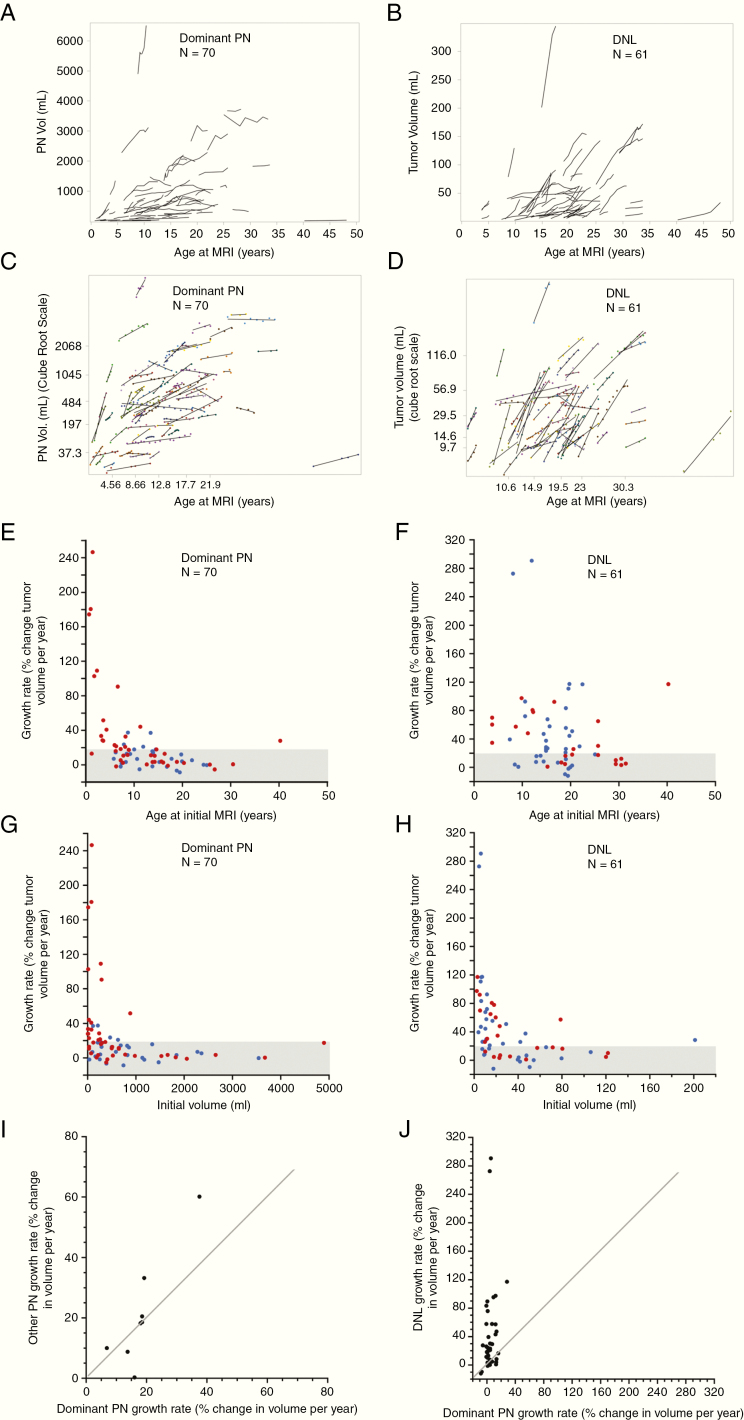
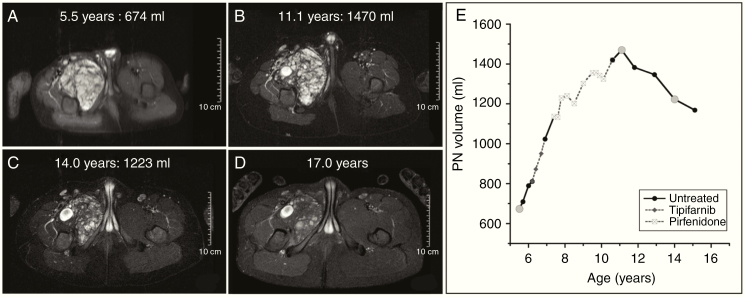
Results: DNLs were observed in 58/122 (45.6%) patients (median 2 DNLs/patient). In DNLs that developed during follow-up, median age of development was 17 years. A moderate negative correlation was observed between the estimated PN growth rate and patients' age at initial MRI (Spearman's r [95% CI]: -0.60 [-0.73, -0.43], n = 70), whereas only a weak correlation was observed for DNLs (Spearman's r [95% CI]: -0.25 [-0.47, 0.004]; n = 61). We observed a moderate negative correlation between tumor growth rate and baseline tumor volume for PNs and DNLs (Spearman's r [95% CI]: -0.52 [-0.67, -0.32] and -0.61 [-0.75, -0.42], respectively). Spontaneous tumor volume reduction was observed in 10 PNs and 7 DNLs (median decrease per year, 3.6% and 7.3%, respectively).
Conclusion: We corroborate previously described findings that most rapidly growing PNs are observed in young children. DNLs tend to develop later in life and their growth is minimally age related. Distinct growth characteristics of PNs and DNLs suggest that these lesions have a different biology and may require different clinical management and clinical trial design. In a subset of PNs and DNLs, slow spontaneous regression in tumor volume was seen.
Keywords: atypical neurofibroma; neurofibromatosis; plexiform neurofibroma; volumetric MRI.
Published by Oxford University Press on behalf of the Society for Neuro-Oncology 2020.
Figures
References
-
- Korf BR. Plexiform neurofibromas. Am J Med Genet. 1999;89(1): 31–37. - PubMed
-
- Nguyen R, Kluwe L, Fuensterer C, Kentsch M, Friedrich RE, Mautner VF. Plexiform neurofibromas in children with neurofibromatosis type 1: frequency and associated clinical deficits. J Pediatr. 2011;159:652–655.e652. - PubMed
-
- Dombi E, Solomon J, Gillespie AJ, et al. . NF1 plexiform neurofibroma growth rate by volumetric MRI: relationship to age and body weight. Neurology. 2007;68(9):643–647. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
