

The role of phenotype on ventilation and exercise capacity in patients affected by COPD: a retrospective study
- PMID: 32153779
- PMCID: PMC7037504
- DOI: 10.4081/mrm.2020.476
The role of phenotype on ventilation and exercise capacity in patients affected by COPD: a retrospective study
Abstract
Background: The idea of phenotype in chronic obstructive pulmonary disease (COPD) has evolved in the last decades, and the importance of peculiar treatment strategies has now been acknowledged. Although dyspnea and exercise limitation are hallmarks of COPD, this aspect has never been fully explored in literature in terms of disease phenotype. The aim of the present study was to explore the relevance of clinical COPD phenotypes on exercise ventilation and maximal capacity.
Methods: In this observational cohort retrospective study we analyzed the data of 50 COPD patients who underwent cardiopulmonary exercise test, categorized as emphysematous (n=29), and non-emphysematous (n=21) according to a previously validated model.
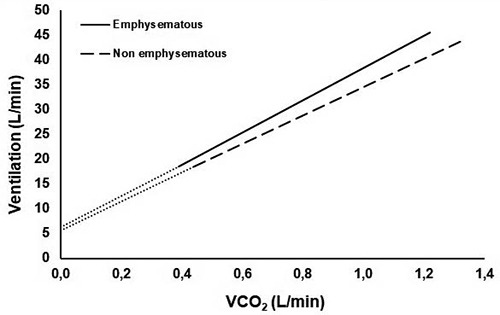
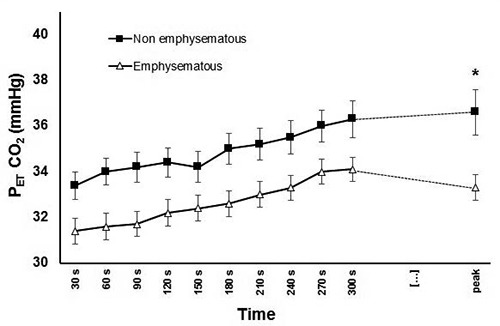
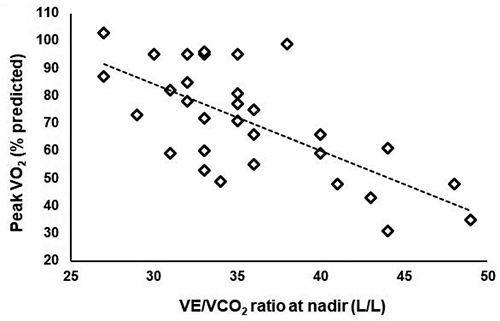
Results: We found a significant difference in terms of VE/VCO2 slope (median values 32.4 vs 28.0, p=0.015) and VE/VCO2 ratio at nadir (median values 37 vs. 33, p=0.004), which resulted higher in emphysematous patients, who also presented lower PETCO2 values (median values 32.6 vs 35.6, p=0.008). In a subgroup of 31 tests which met the maximality criteria, emphysematous patients presented a significantly lower work rate at peak (median value 51 vs 72% predicted, p=0.016), and showed a lower peak oxygen consumption, although at the limit of significance (median values of 63 vs 85 % predicted, p=0.051).
Conclusions: This study extends our knowledge about the characterization of the COPD phenotypical expression of disease, showing that patients affected by emphysema are more prone to ventilatory inefficiency during exercise, and that this is likely to be an important cause of their overall reduced exercise capacity.
Keywords: COPD; cardiopulmonary exercise test; emphysema; exercise capacity; phenotype; ventilation.
©Copyright: the Author(s), 2020.
Conflict of interest statement
Conflict of interest: The Authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous