

The effect of culinary interventions (cooking classes) on dietary intake and behavioral change: a systematic review and evidence map
- PMID: 32153942
- PMCID: PMC7050805
- DOI: 10.1186/s40795-019-0293-8
The effect of culinary interventions (cooking classes) on dietary intake and behavioral change: a systematic review and evidence map
Abstract
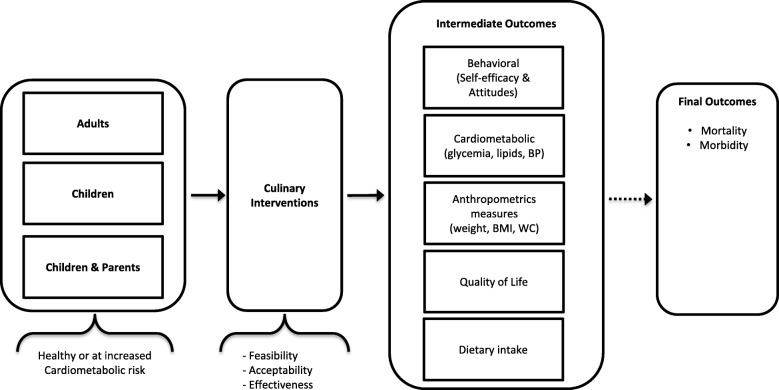
Background: Culinary interventions (cooking classes) have been used to improve the quality of dietary intake and change behavior. The aim of this systematic review is to investigate the effects of culinary interventions on dietary intake and behavioral and cardiometabolic outcomes.
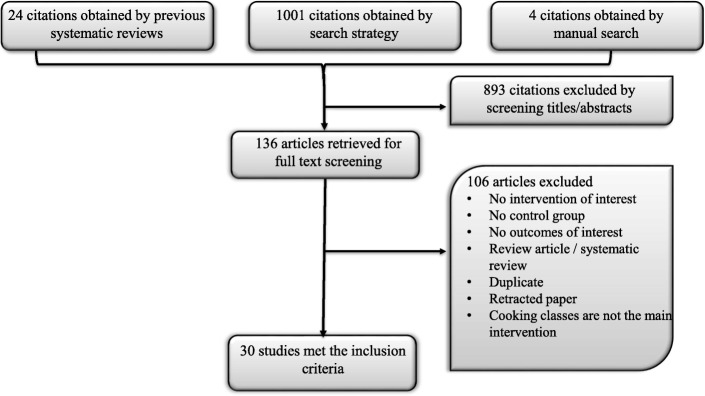
Methods: We conducted a systematic review of MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and Scopus for comparative studies that evaluated culinary interventions to a control group or baseline values. The intervention was defined as a cooking class regardless of its length or delivery approach. Studies included populations of children, healthy adults or adults with morbidities. The risk of bias was assessed using the Cochrane Risk of Bias tool and the Newcastle-Ottawa Scale. Outcomes were pooled using the random-effects model and descriptive statistics and depicted in an evidence map. Simple logistic regression was used to evaluate factors associated with intervention success.
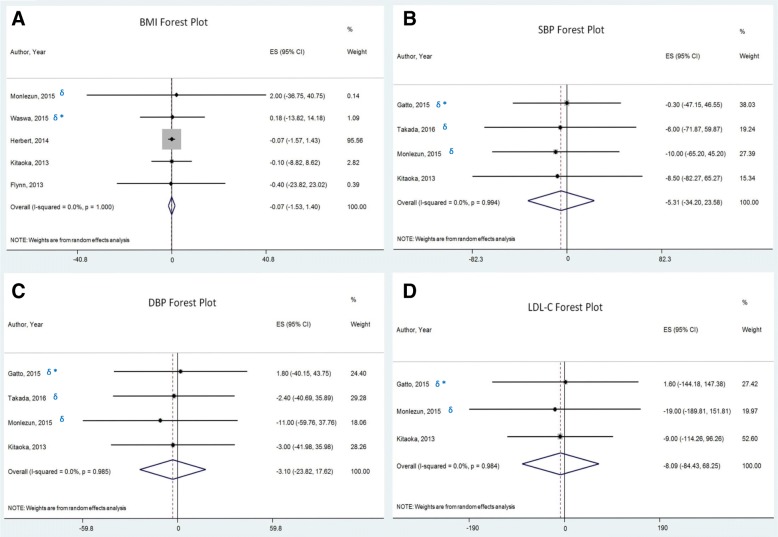
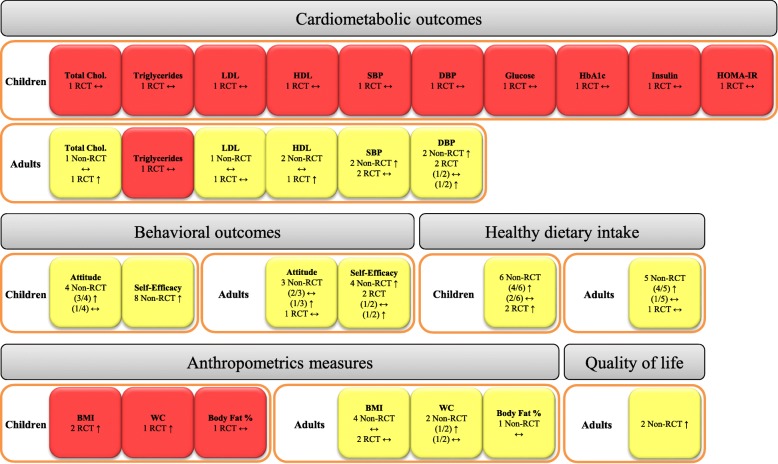
Results: We included 30 studies (6 were randomized, 7381 patients, average follow up 25 weeks). Culinary interventions were not associated with a significant change in body mass index (- 0.07 kg/m2, 95% CI: -1.53, 1.40), systolic (- 5.31 mmHg, 95% CI: -34.2, 23.58) or diastolic blood pressure (- 3.1 mmHg, 95% CI: -23.82, 17.62) or LDL cholesterol (- 8.09 mg/dL, 95% CI: -84.43, 68.25). Culinary interventions were associated with improved attitudes, self-efficacy and healthy dietary intake in adults and children. We were unable to demonstrate whether the effect of a culinary intervention was modified by various characteristics of the intervention such as its delivery or intensity. Interventions with additional components such as education on nutrition, physical activity or gardening were particularly effective.
Conclusions: Culinary interventions were not associated with a significant change in cardiometabolic risk factors, but were associated with improved attitudes, self-efficacy and a healthier dietary intake in adults and children.
Keywords: Chronic disease prevention; Cooking classes; Culinary intervention; Dietary intake; Evidence map; Nutrition; Systematic review.
© The Author(s). 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- Schwingshackl L, Schwedhelm C, Hoffmann G, Lampousi AM, Knuppel S, Iqbal K, Bechthold A, Schlesinger S, Boeing H. Food groups and risk of all-cause mortality: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr. 2017;105(6):1462–1473. - PubMed
-
- Van Horn L, Carson JA, Appel LJ, Burke LE, Economos C, Karmally W, Lancaster K, Lichtenstein AH, Johnson RK, Thomas RJ, et al. Recommended dietary pattern to achieve adherence to the American Heart Association/American College of Cardiology (AHA/ACC) guidelines: a scientific statement from the American Heart Association. Circulation. 2016;134(22):e505–e529. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, et al. Heart disease and stroke Statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603. doi: 10.1161/CIR.0000000000000485. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Medical