

Electrocardiograms for cardiomyopathy risk stratification in children with anthracycline exposure
- PMID: 32154016
- PMCID: PMC7048097
- DOI: 10.1186/s40959-019-0045-6
Electrocardiograms for cardiomyopathy risk stratification in children with anthracycline exposure
Abstract
Background: Early recognition of anthracycline-induced cardiomyopathy may reduce morbidity and mortality in children, but risk stratification tools are lacking. This study evaluates whether electrocardiogram (ECG) changes precede echocardiographic abnormalities in children with anthracycline-induced cardiomyopathy.
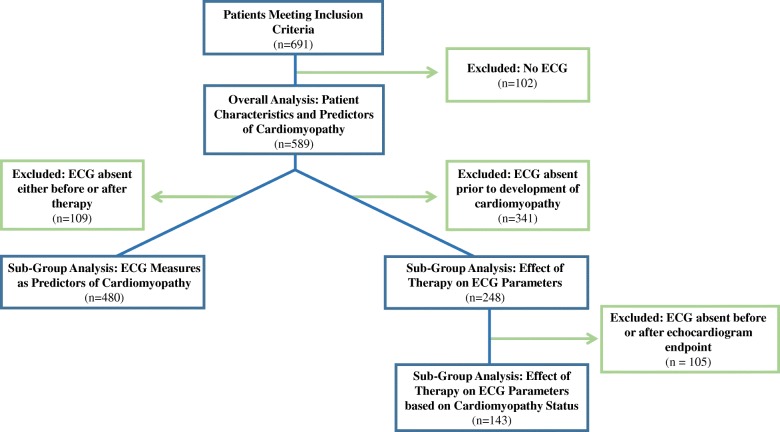
Methods: We performed a retrospective analysis of 589 pediatric cancer patients who received anthracyclines at a tertiary referral center. ECG endpoints were sum of absolute QRS amplitudes in the 6 limb leads (ΣQRS(6 L)) and corrected QT interval (QTc). Cardiomyopathy was defined by echocardiogram as ejection fraction < 50%, shortening fraction < 26%, or left ventricular end-diastolic diameter z-score > 2.5.
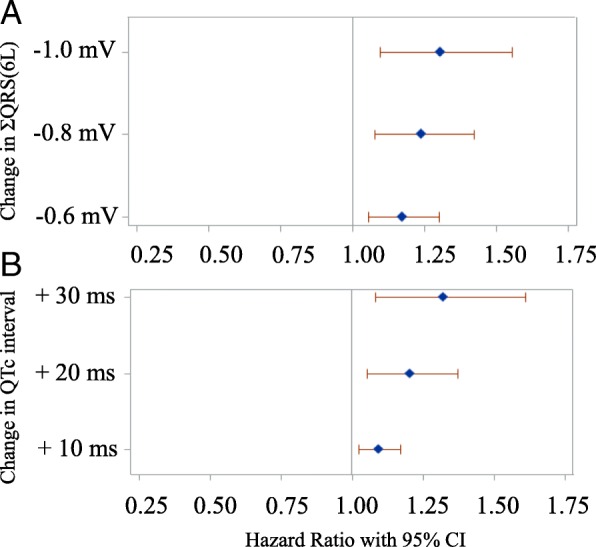
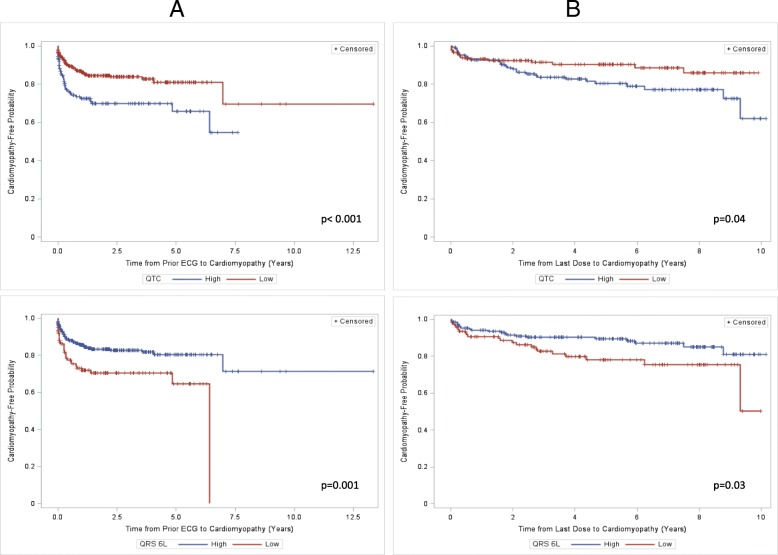
Results: Median age at start of therapy was 7.8 years (IQR 3.7-13.6); median follow-up time was 3.6 years (IQR 1.1-5.8). 19.5% of patients met criteria for cardiomyopathy. Male sex, race, older age at first dose, and larger body surface area were associated with development of cardiomyopathy. A 0.6 mV decrease in ΣQRS(6 L) and 10 ms increase in QTc were associated with an increased risk of developing cardiomyopathy with hazard ratios of 1.174 (95% CI = 1.057-1.304, p = 0.003) and 1.098 (95%CI = 1.027-1.173, p = 0.006) respectively. Kaplan-Meier estimates showed a lower chance of cardiomyopathy-free survival for QTc ≥ 440 ms and ΣQRS(6 L) ≤ 3.2 mV over time. After controlling for confounders, total anthracycline dose predicted a decrease in ΣQRS(6 L) and an increase in QTc independent of cardiomyopathy status (p = 0.01 and p < 0.001 respectively). Cardiotoxic radiation did not predict changes in ECG parameters. Cardiomyopathy was associated with increased mortality (34% versus 12%, p < 0.001).
Conclusion: In children receiving anthracyclines, decrease in ΣQRS(6 L) and QTc prolongation are associated with increased risk of developing cardiomyopathy. ECG is a potential non-invasive risk stratification tool for prediction of anthracycline-induced cardiomyopathy and requires prospective validation.
Keywords: Anthracyclines; Cardiomyopathy; Electrocardiograms; Pediatric oncology.
© The Author(s). 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures

References
-
- Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, Hudson MM, Kremer LC, Landy DC, Miller TL, Oeffinger KC, Rosenthal DN, Sable CA, Sallan SE, Singh GK, Steinberger J, Cochran TR, Wilkinson JD. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy. Circulation. 2013;128:1927–1995. doi: 10.1161/CIR.0b013e3182a88099. - DOI - PubMed
-
- Shankar SM, Marina N, Hudson MM, Hodgson DC, Adams MJ, Landier W, Bhatia S, Meeske K, Hui Chen M, Kinahan KE, Steinberger J, Rosenthal D. Monitoring for cardiovascular disease in survivors of childhood cancer: report from the cardiovascular disease task force of the children’s oncology group. Pediatrics. 2008;121:e387–e396. doi: 10.1542/peds.2007-0575. - DOI - PubMed
-
- Lipshultz SE, Lipsitz SR, Mone SM, Goorin AM, Sallan SE, Sanders SP, Orav EJ, Gelber RD, Colan SD. Female sex and higher drug dose as risk factors for late cardiotoxic effects of doxorubicin therapy for childhood cancer. N Engl J Med. 1995;332:1738–1743. doi: 10.1056/NEJM199506293322602. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous