

Evaluation of Renal Safety Between Imipenem/Relebactam and Colistin Plus Imipenem in Patients With Imipenem-Nonsusceptible Bacterial Infections in the Randomized, Phase 3 RESTORE-IMI 1 Study
- PMID: 32154325
- PMCID: PMC7052751
- DOI: 10.1093/ofid/ofaa054
Evaluation of Renal Safety Between Imipenem/Relebactam and Colistin Plus Imipenem in Patients With Imipenem-Nonsusceptible Bacterial Infections in the Randomized, Phase 3 RESTORE-IMI 1 Study
Abstract
Background: In the randomized controlled RESTORE-IMI 1 clinical trial (NCT02452047), imipenem/cilastatin (IMI) with relebactam (IMI/REL) was as effective as colistin plus IMI for the treatment of imipenem-nonsusceptible gram-negative infections. Differences in nephrotoxicity were observed between treatment arms. As there is no standard definition of nephrotoxicity used in clinical trials, we conducted analyses to further understand the renal safety profile of both treatments.
Methods: Nephrotoxicity was retrospectively evaluated using 2 acute kidney injury assessment criteria (Kidney Disease Improving Global Outcomes [KDIGO] and Risk, Injury, Failure, Loss, and End-stage Kidney Disease [RIFLE]). Additional outcomes included time to onset of protocol-defined nephrotoxicity and incidence of renal adverse events.
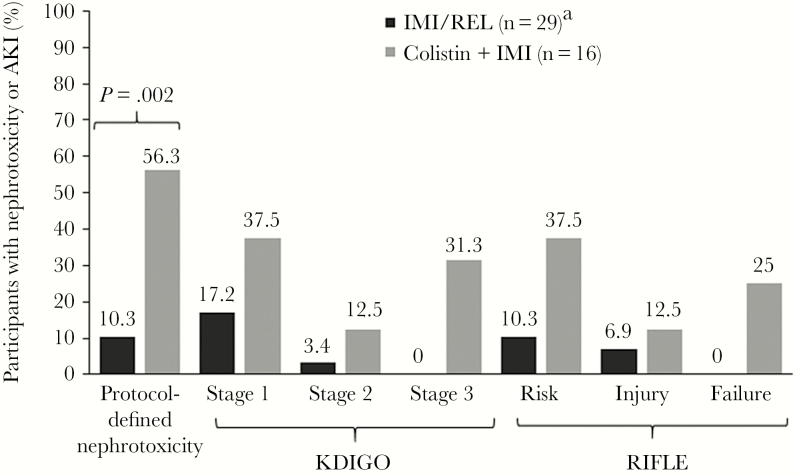
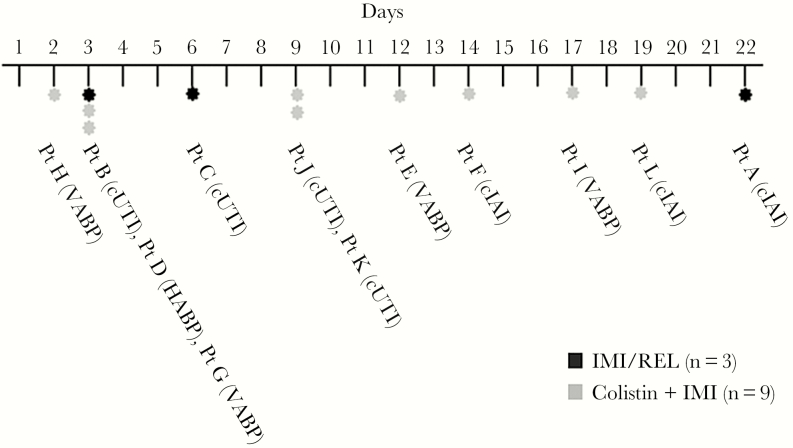
Results: Of 47 participants receiving treatment, 45 had sufficient data to assess nephrotoxicity (IMI/REL, n = 29; colistin plus IMI, n = 16). By KDIGO criteria, no participants in the IMI/REL but 31.3% in the colistin plus IMI group experienced stage 3 acute kidney injury. No IMI/REL-treated participants experienced renal failure by RIFLE criteria, vs 25.0% for colistin plus IMI. Overall, the time to onset of nephrotoxicity varied considerably (2-22 days). Fewer renal adverse events (12.9% vs 37.5%), including discontinuations due to drug-related renal adverse events (0% vs 12.5%), were observed in the IMI/REL group compared with the colistin plus IMI group, respectively.
Conclusions: Our analyses confirm the findings of a preplanned end point and provide further evidence that IMI/REL had a more favorable renal safety profile than colistin-based therapy in patients with serious, imipenem-nonsusceptible gram-negative bacterial infections.
Clinicaltrialsgov identifier: NCT02452047.
Keywords: IMI/REL; KDIGO criteria; RIFLE criteria; acute kidney injury; colistin.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Available at: https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf Accessed 17 August 2018.
-
- Judd WR, Ratliff PD, Hickson RP, et al. . Clinical and economic impact of meropenem resistance in Pseudomonas aeruginosa-infected patients. Am J Infect Control 2016; 44:1275–9. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
