

Attenuation of MODS-related and ARDS-related mortality makes infectious complications a remaining challenge in the severely injured
- PMID: 32154377
- PMCID: PMC7046953
- DOI: 10.1136/tsaco-2019-000398
Attenuation of MODS-related and ARDS-related mortality makes infectious complications a remaining challenge in the severely injured
Abstract
Introduction: The recent decrease in multiple organ dysfunction syndrome (MODS)-associated and adult respiratory distress syndrome (ARDS)-associated mortality could be considered a success of improvements in trauma care. However, the incidence of infections remains high in patients with polytrauma, with high morbidity and hospital resources usage. Infectious complications might be a residual effect of the decrease in MODS-related/ARDS-related mortality. This study investigated the current incidence of infectious complications in polytrauma.
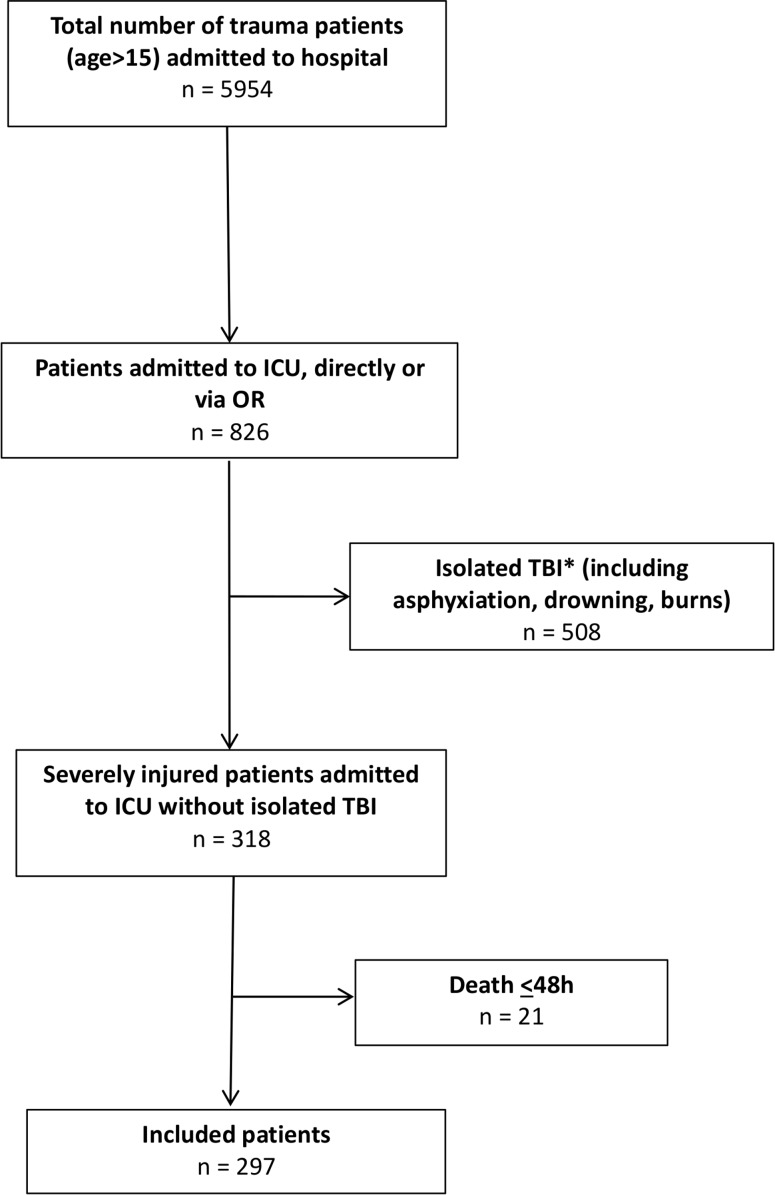
Methods: A 5.5-year prospective population-based cohort study included consecutive severely injured patients (age >15) admitted to a (Level-1) trauma center intensive care unit (ICU) who survived >48 hours. Demographics, physiologic and resuscitation parameters, multiple organ failure and ARDS scores, and infectious complications (pneumonia, fracture-related infection, meningitis, infections related to blood, wound, and urinary tract) were prospectively collected. Data are presented as median (IQR), p<0.05 was considered significant.
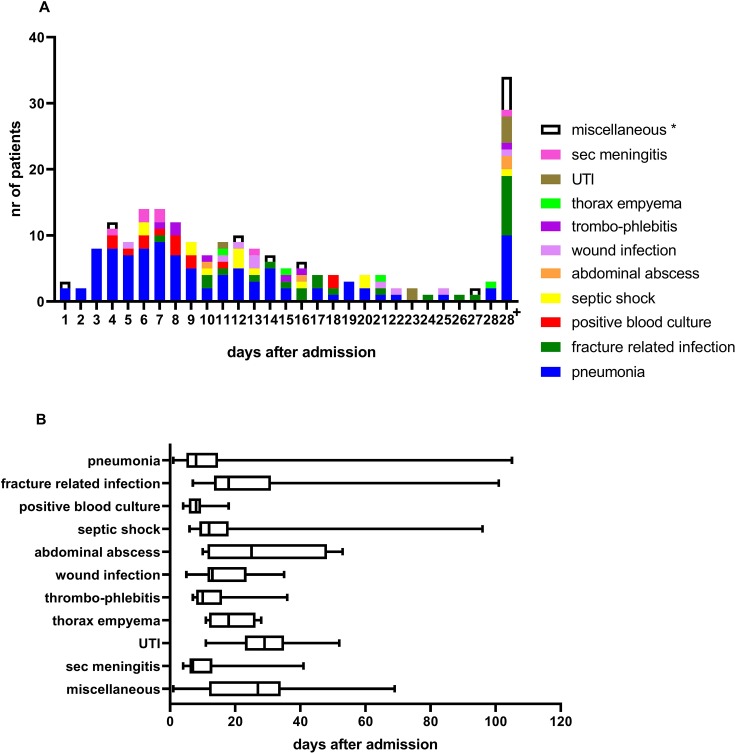
Results: 297 patients (216 (73%) men) were included with median age of 46 (27-60) years, median Injury Severity Score was 29 (22-35), 96% sustained blunt injuries. 44 patients (15%) died. One patient (2%) died of MODS and 1 died of ARDS. 134 patients (45%) developed 201 infectious complications. Pneumonia was the most common complication (50%). There was no difference in physiologic parameters on arrival in emergency department and ICU between patients with and without infectious complications. Patients who later developed infections underwent more often a laparotomy (32% vs 18%, p=0.009), had more often pelvic fractures (38% vs 25%, p=0.02), and received more blood products <8 hours. They had more often MODS (25% vs 13%, p=0.005), stayed longer on the ventilator (10 (5-15) vs 5 (2-8) days, p<0.001), longer in ICU (11 (6-17) vs 6 (3-10) days, p<0.001), and in hospital (30 (20-44) vs 16 (10-24) days, p<0.001). There was however no difference in mortality (12% vs 17%, p=0.41) between both groups.
Conclusion: 45% of patients developed infectious complications. These patients had similar mortality rates, but used more hospital resources. With low MODS-related and ARDS-related mortality, infections might be a residual effect, and are one of the remaining challenges in the treatment of patients with polytrauma.
Level of evidence: Level 3.
Study type: Population-based cohort study.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Dilemma of crystalloid resuscitation in non-exsanguinating polytrauma: what is too much?Trauma Surg Acute Care Open. 2020 Oct 28;5(1):e000593. doi: 10.1136/tsaco-2020-000593. eCollection 2020. Trauma Surg Acute Care Open. 2020. PMID: 33178897 Free PMC article.
-
Reduction in Mortality Rates of Postinjury Multiple Organ Dysfunction Syndrome: A Shifting Paradigm? A Prospective Population-Based Cohort Study.Shock. 2018 Jan;49(1):33-38. doi: 10.1097/SHK.0000000000000938. Shock. 2018. PMID: 28682941
-
Incidence of acute respiratory distress syndrome and associated mortality in a polytrauma population.Trauma Surg Acute Care Open. 2018 Dec 19;3(1):e000232. doi: 10.1136/tsaco-2018-000232. eCollection 2018. Trauma Surg Acute Care Open. 2018. PMID: 30623025 Free PMC article.
-
Using IL-6 concentrations in the first 24 h following trauma to predict immunological complications and mortality in trauma patients: a meta-analysis.Eur J Trauma Emerg Surg. 2018 Oct;44(5):679-687. doi: 10.1007/s00068-017-0880-9. Epub 2017 Nov 14. Eur J Trauma Emerg Surg. 2018. PMID: 29138874 Review.
-
[Gene polymorphism in intensive care patients. Is the course of disease predetermined?].Anaesthesist. 2004 Mar;53(3):213-27. doi: 10.1007/s00101-004-0654-8. Anaesthesist. 2004. PMID: 15021953 Free PMC article. Review. German.
Cited by
-
Visualization of the inflammatory response to injury by neutrophil phenotype categories : Neutrophil phenotypes after trauma.Eur J Trauma Emerg Surg. 2023 Apr;49(2):1023-1034. doi: 10.1007/s00068-022-02134-3. Epub 2022 Nov 8. Eur J Trauma Emerg Surg. 2023. PMID: 36348032 Free PMC article.
-
Geriatric polytrauma patients should not be excluded from aggressive injury treatment based on age alone.Eur J Trauma Emerg Surg. 2022 Feb;48(1):357-365. doi: 10.1007/s00068-020-01567-y. Epub 2020 Dec 15. Eur J Trauma Emerg Surg. 2022. PMID: 33320284 Free PMC article.
-
Anion gap predicting 90-Day mortality and guiding furosemide use in ARDS.Sci Rep. 2025 Feb 10;15(1):4954. doi: 10.1038/s41598-025-89163-1. Sci Rep. 2025. PMID: 39930113 Free PMC article.
-
Pneumonia in the first week after polytrauma is associated with reduced blood levels of soluble herpes virus entry mediator.Front Immunol. 2023 Dec 22;14:1259423. doi: 10.3389/fimmu.2023.1259423. eCollection 2023. Front Immunol. 2023. PMID: 38187375 Free PMC article.
-
Dilemma of crystalloid resuscitation in non-exsanguinating polytrauma: what is too much?Trauma Surg Acute Care Open. 2020 Oct 28;5(1):e000593. doi: 10.1136/tsaco-2020-000593. eCollection 2020. Trauma Surg Acute Care Open. 2020. PMID: 33178897 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials