

Alternative clinical trial designs
- PMID: 32154379
- PMCID: PMC7046952
- DOI: 10.1136/tsaco-2019-000420
Alternative clinical trial designs
Abstract
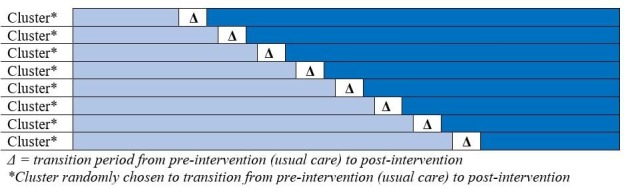
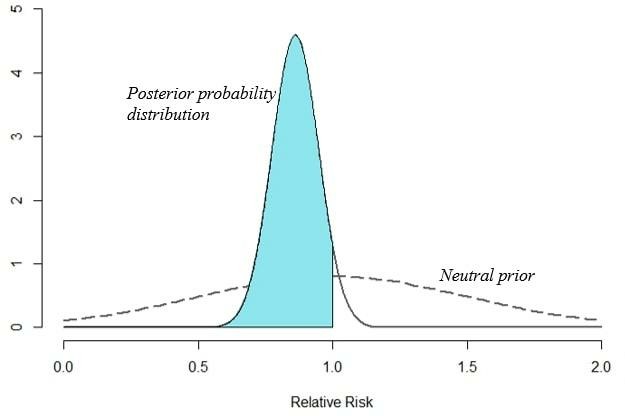
High-quality clinical trials are needed to advance the care of injured patients. Traditional randomized clinical trials in trauma have challenges in generating new knowledge due to many issues, including logistical difficulties performing individual randomization, unclear pretrial estimates of treatment effect leading to often unpowered studies, and difficulty assessing the generalizability of an intervention given the heterogeneity of both patients and trauma centers. In this review, we discuss alternative clinical trial designs that can address some of these difficulties. These include pragmatic trials, cluster randomization, cluster randomized stepped wedge designs, factorial trials, and adaptive designs. Additionally, we discuss how Bayesian methods of inference may provide more knowledge to trauma and acute care surgeons compared with traditional, frequentist methods.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma. JAMA 2015;313:471–82. 10.1001/jama.2015.12 - DOI - PMC - PubMed
-
- Bhullar IS, Frykberg ER, Tepas JJ, Siragusa D, Loper T, Kerwin AJ. At first blush: absence of computed tomography contrast extravasation in grade IV or V adult blunt splenic trauma should not preclude angioembolization. J Trauma Acute Care Surg 2013;74:105–11. discussion 11-2 10.1097/TA.0b013e3182788cd2 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources