

Functional complaints and quality of life after transanal total mesorectal excision: a meta-analysis
- PMID: 32154594
- PMCID: PMC7155085
- DOI: 10.1002/bjs.11566
Functional complaints and quality of life after transanal total mesorectal excision: a meta-analysis
Abstract
Background: Total mesorectal excision (TME) gives excellent oncological results in rectal cancer treatment, but patients may experience functional problems. A novel approach to performing TME is by single-port transanal minimally invasive surgery. This systematic review evaluated the functional outcomes and quality of life after transanal and laparoscopic TME.
Methods: A comprehensive search in PubMed, the Cochrane Library, Embase and the trial registers was conducted in May 2019. PRISMA guidelines were used. Data for meta-analysis were pooled using a random-effects model.
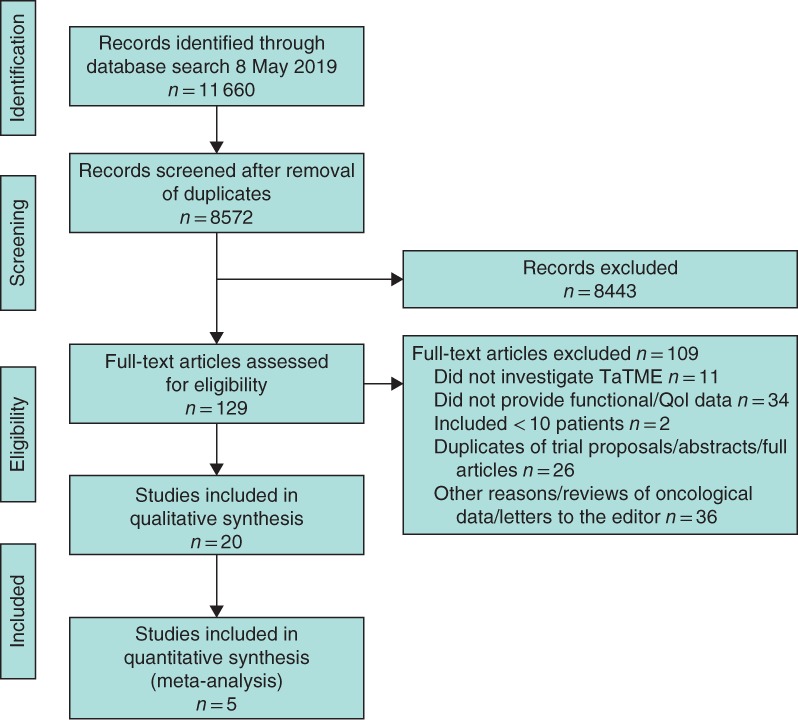
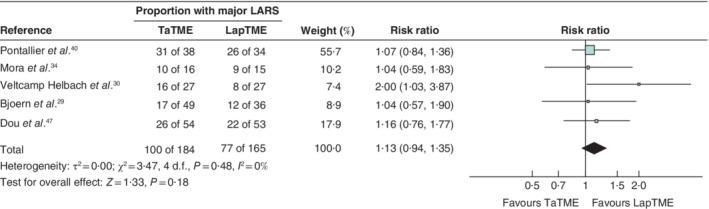
Results: A total of 11 660 studies were identified, from which 14 studies and six conference abstracts involving 846 patients (599 transanal TME, 247 laparoscopic TME) were included. A substantial number of patients experienced functional problems consistent with low anterior resection syndrome (LARS). Meta-analysis found no significant difference in major LARS between the two approaches (risk ratio 1·13, 95 per cent c.i. 0·94 to 1·35; P = 0·18). However, major heterogeneity was present in the studies together with poor reporting of functional baseline assessment.
Conclusion: No differences in function were observed between transanal and laparoscopic TME.
Antecedentes: La escisión total del mesorrecto (total mesorectal excision, TME) proporciona excelentes resultados oncológicos en el tratamiento del cáncer de recto, pero los pacientes pueden presentar trastornos funcionales. Un abordaje novedoso para realizar la TME es mediante cirugía transanal mínimamente invasiva de puerto único. En esta revisión sistemática se evaluaron los resultados funcionales y la calidad de vida después de TME transanal (TaTME) y TME laparoscópica (LapTME). MÉTODOS: En mayo de 2019 se realizó una búsqueda exhaustiva en las bases de datos de Pubmed, Biblioteca Cochrane, EMBASE y en los registros de ensayos clínicos. Se utilizaron las guías PRISMA. Los datos para el metaanálisis se agruparon utilizando un modelo de efectos aleatorios.
Resultados: Se identificaron un total de 11.660 estudios, de los cuales se incluyeron 14 estudios y 6 resúmenes de congresos con 846 pacientes (599 TaTME/247 LapTME). Un número sustancial de pacientes presentó trastornos funcionales consistentes con el síndrome de resección anterior baja (low anterior resection syndrome, LARS). El metaanálisis no encontró diferencias significativas en los porcentajes de LARS grave entre los dos abordajes (razón de oportunidades, odds ratio, OR 1,13; i.c. del 95% 0,94-1,35; P = 0,18). Sin embargo, los estudios globalmente presentaron una gran heterogeneidad, así como una deficiente información sobre la evaluación funcional basal. CONCLUSIÓN: No se observaron diferencias en la función entre TaTME y LapTME.
© 2020 BJS Society Ltd published by John Wiley & Sons Ltd.
Figures
References
-
- Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ et al.; COlon cancer Laparoscopic or Open Resection Study Group (COLOR). Laparoscopic surgery versus open surgery for colon cancer: short‐term outcomes of a randomised trial. Lancet Oncol 2005; 6: 477–484. - PubMed
-
- Kang SB, Park JW, Jeong SY, Nam BH, Choi HS, Kim DW et al Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): short‐term outcomes of an open‐label randomised controlled trial. Lancet Oncol 2010; 11: 637–645. - PubMed
-
- Jeong SY, Park JW, Nam BH, Kim S, Kang SB, Lim SB et al Open versus laparoscopic surgery for mid‐rectal or low‐rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open‐label, non‐inferiority, randomised controlled trial. Lancet Oncol 2014; 15: 767–774. - PubMed
-
- Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ. Five‐year follow‐up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 2010; 97: 1638–1645. - PubMed
