

Peripheral endothelial dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome
- PMID: 32154656
- PMCID: PMC7261521
- DOI: 10.1002/ehf2.12633
Peripheral endothelial dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome
Abstract
Aims: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a complex multisystem disease. Evidence for disturbed vascular regulation comes from various studies showing cerebral hypoperfusion and orthostatic intolerance. The peripheral endothelial dysfunction (ED) has not been sufficiently investigated in patients with ME/CFS. The aim of the present study was to examine peripheral endothelial function in patients with ME/CFS.
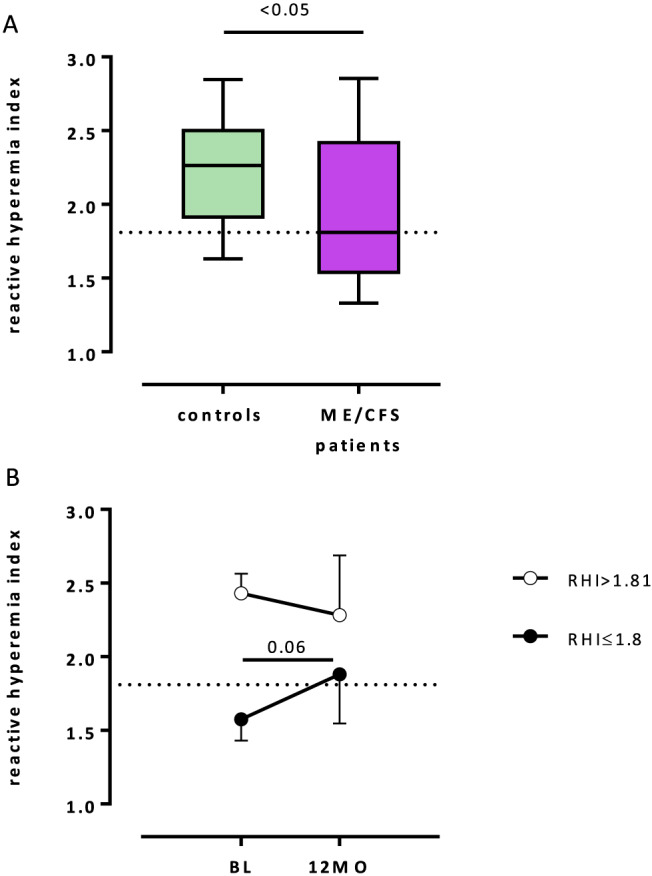
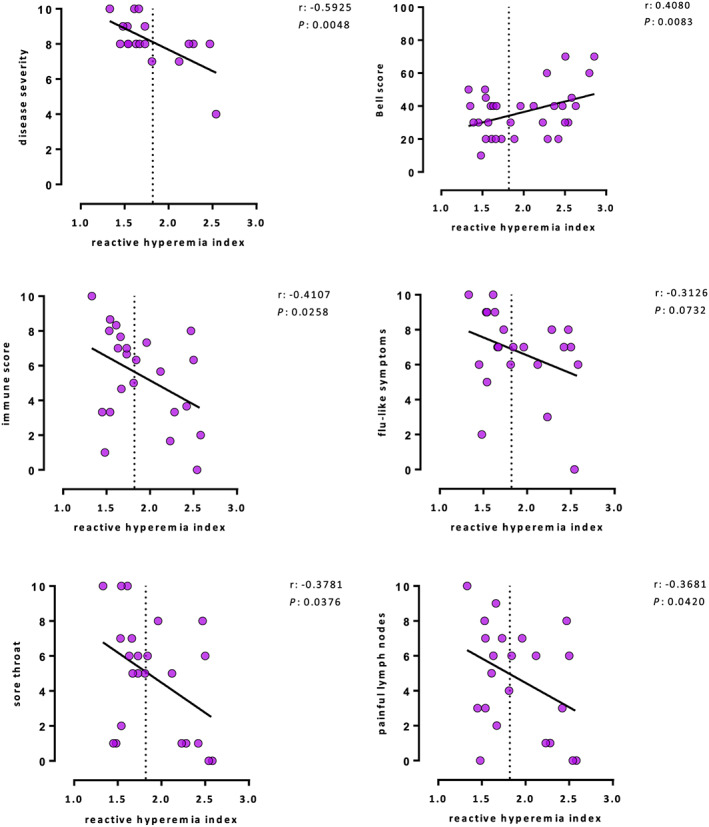
Methods and results: Thirty-five patients [median age 40 (range 18-70) years, mean body mass index 23.8 ± 4.2 kg/m2 , 31% male] with ME/CFS were studied for peripheral endothelial function assessed by peripheral arterial tonometry (EndoPAT2000). Clinical diagnosis of ME/CFS was based on Canadian Criteria. Nine of these patients with elevated antibodies against β2-adrenergic receptor underwent immunoadsorption, and endothelial function was measured at baseline and 3, 6, and 12 months follow-up. ED was defined by reactive hyperaemia index ≤1.81. Twenty healthy subjects of similar age and body mass index were used as a control group. Peripheral ED was found in 18 of 35 patients (51%) with ME/CFS and in 4 healthy subjects (20%, P < 0.05). Patients with ED, in contrast to patients with normal endothelial function, reported more severe disease according to Bell score (31 ± 12 vs. 40 ± 16, P = 0.04), as well as more severe fatigue-related symptoms (8.62 ± 0.87 vs. 7.75 ± 1.40, P = 0.04) including a higher demand for breaks [9.0 (interquartile range 7.0-10.0) vs. 7.5 (interquartile range 6.0-9.25), P = 0.04]. Peripheral ED showed correlations with more severe immune-associated symptoms (r = -0.41, P = 0.026), such as sore throat (r = -0.38, P = 0.038) and painful lymph nodes (r = -0.37, P = 0.042), as well as more severe disease according to Bell score (r = 0.41, P = 0.008) and symptom score (r = -0.59, P = 0.005). There were no differences between the patient group with ED and the patient group with normal endothelial function regarding demographic, metabolic, and laboratory parameters. Further, there was no difference in soluble vascular cell adhesion molecule and soluble intercellular adhesion molecule levels. At baseline, peripheral ED was observed in six patients who underwent immunoadsorption. After 12 months, endothelial function had improved in five of these six patients (reactive hyperaemia index 1.58 ± 0.15 vs. 2.02 ± 0.46, P = 0.06).
Conclusions: Peripheral ED is frequent in patients with ME/CFS and associated with disease severity and severity of immune symptoms. As ED is a risk factor for cardiovascular disease, it is important to elucidate if peripheral ED is associated with increased cardiovascular morbidity and mortality in ME/CFS.
Keywords: Cardiovascular risk factor; Chronic fatigue syndrome; Immune score; Peripheral endothelial dysfunction; Reactive hyperaemia index.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Carruthers BM, van de Sande MI, De Meirleir KL, Klimas NG, Broderick G, Mitchell T, Staines D, Powles AC, Speight N, Vallings R, Bateman L, Baumgarten‐Austrheim B, Bell DS, Carlo‐Stella N, Chia J, Darragh A, Jo D, Lewis D, Light AR, Marshall‐Gradisnik S, Mena I, Mikovits JA, Miwa K, Murovska M, Pall ML, Stevens S. Myalgic encephalomyelitis: international consensus criteria. J Intern Med 2011; 270: 327–338. - PMC - PubMed
-
- Newton JL, Okonkwo O, Sutcliffe K, Seth A, Shin J, Jones DE. Symptoms of autonomic dysfunction in chronic fatigue syndrome. QJM 2007; 100: 519–526. - PubMed
-
- Sotzny F, Blanco J, Capelli E, Castro‐Marrero J, Steiner S, Murovska M. Scheibenbogen C; European Network on ME/CFS (EUROMENE). Autoimmun Rev 2018; 17: 601–609. - PubMed
-
- Scherbakov N, Sandek A, Martens‐Lobenhoffer J, Kung T, Turhan G, Liman T, Ebinger M, von Haehling S, Bode‐Böger SM, Endres M, Doehner W. Endothelial dysfunction of the peripheral vascular bed in the acute phase after ischemic stroke. Cerebrovasc Dis 2012; 33: 37–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
