

Association of Disease Progression With Health-Related Quality of Life Among Adults With Breast, Lung, Pancreatic, and Colorectal Cancer
- PMID: 32154886
- PMCID: PMC7064873
- DOI: 10.1001/jamanetworkopen.2020.0643
Association of Disease Progression With Health-Related Quality of Life Among Adults With Breast, Lung, Pancreatic, and Colorectal Cancer
Abstract
Importance: Mortality, morbidity, and health-related quality of life (HRQoL) are patient-relevant end points generally considered in the early benefit assessments of new cancer treatments. Progression-related end points, such as time to progression or progression-free survival, are not included, although patients and physicians testify to the detrimental association of disease progression with HRQoL.
Objective: To examine the association of disease progression and HRQoL in 4 prevalent solid-cancer entities in routine clinical practice.
Design, setting, and participants: This cohort study evaluated data from 4 prospective, nonintervention, multicenter registries collected between 2011 and 2018 in 203 centers in Germany. Patients' HRQoL was assessed regularly for up to 5 years. The change in HRQoL scores after disease progression was examined with linear mixed models, adjusting for demographic and clinical covariates. Patients with metastatic breast, pancreatic, lung, and colorectal cancer were recruited at the start of systemic first-line treatment. Data analysis was performed from February 2019 to April 2019.
Exposures: All patients received systemic, palliative first-line treatment according to their physician's choice.
Main outcomes and measures: The primary outcome was deterioration of HRQoL associated with disease progression, as measured by 4 validated questionnaires: Functional Assessment of Cancer Therapy-General version 4, European Organization for Research and Treatment of Cancer QLQ-C30 version 3.0, European Organization for Research and Treatment of Cancer QLQ-C15-PAL version 1, and Hospital Anxiety and Depression Scale.
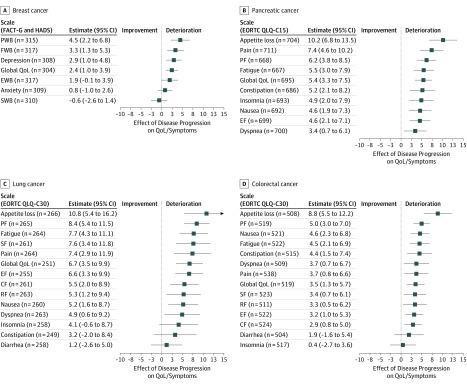
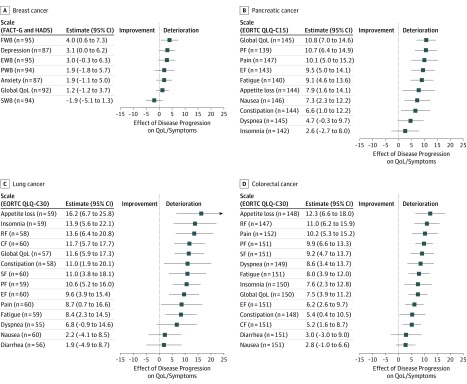
Results: More than 8000 questionnaires from 2314 patients with 2562 documented disease progressions were analyzed. In total, 464 patients had breast cancer (464 [100.0%] female; median [range] age, 61.6 [26.4-90.1] years), 807 patients had pancreatic cancer (352 [43.6%] female; median [range] age, 70.0 [39.0-93.0] years), 341 patients had lung cancer (118 [34.6%] female; median [range] age, 65.9 [28.4-88.2] years), and 702 patients had colorectal cancer (248 [35.3%] female; median [range] age, 66.9 [26.9-92.1] years). The first disease progression was associated with a statistically significant worsening of 37 of 45 HRQoL scales; for 17 of these scales, the worsening was clinically meaningful. Scale scores for appetite loss (pancreatic cancer, 10.2 points [95% CI, 6.8-13.5 points]; lung cancer, 10.8 points [95% CI, 5.4-16.2 points]; colorectal cancer, 8.8 points [95% CI, 5.5-12.2]; all P < .001), physical functioning (pancreatic cancer, 6.2 points [95% CI, 3.8-8.5 points]; lung cancer, 8.4 points [95% CI, 5.4-11.5 points]; colorectal cancer, 5.0 points [95% CI, 3.0-7.0 points]; all P < .001), and fatigue (pancreatic cancer, 5.5 points [95% CI, 3.0-7.9 points]; lung cancer, 7.7 points [95% CI, 4.3-11.1]; colorectal cancer, 4.5 points [95% CI, 2.1-6.9 points]; all P < .001) were most affected, irrespective of the type of cancer. The association with global HRQoL was most pronounced in lung cancer (6.7 points [95% CI, 3.5-9.9 points]; P < .001) and pancreatic cancer (5.4 points [95% CI, 3.3-7.5 points]; P < .001) and less in colorectal cancer (3.5 points [95% CI, 1.3-5.7 points]; P = .002) and breast cancer (2.4 points [95% CI, 1.0-3.9 points]; P = .001). The second progression was associated with an even larger decrease in HRQoL.
Conclusions and relevance: These findings suggest that disease progression is associated with a deterioration in HRQoL among patients with metastatic breast, pancreatic, lung, and colorectal cancer. This evidence highlights the importance of progression-related end points, such as time to progression and progression-free survival, as additional patient-relevant end points when evaluating the benefit of new treatments for patients with metastatic cancer.
Conflict of interest statement
Figures
References
-
- NICE Decision Support Unit, University of Sheffield . Progression-free survival and overall survival (PFS-OS). Accessed May 22, 2019. http://nicedsu.org.uk/methods-development/pfs-os/
-
- Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen . Allgemeine methoden, version 5.0 [in German]. Published July 10, 2017. Accessed May 22, 2019. https://www.iqwig.de/download/Allgemeine-Methoden_Version-5-0.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
