

Absolute risk of tuberculosis among untreated populations with a positive tuberculin skin test or interferon-gamma release assay result: systematic review and meta-analysis
- PMID: 32156698
- PMCID: PMC7190060
- DOI: 10.1136/bmj.m549
Absolute risk of tuberculosis among untreated populations with a positive tuberculin skin test or interferon-gamma release assay result: systematic review and meta-analysis
Abstract
Objective: To determine the annual rate of tuberculosis development after a positive tuberculin skin test (TST) or interferon-gamma release assay result (IGRA), or both, among untreated populations with characteristics believed to increase the risk of tuberculosis (at risk populations).
Design: Systematic review and meta-analysis.
Data sources: Embase, Medline, and Cochrane Controlled Register of Trials from 1 January 1990 to 17 May 2019, for studies in humans published in English or French. Reference lists were reviewed.
Eligibility criteria and data analysis: Retrospective or prospective cohorts and randomised trials that included at least 10 untreated participants who tested positive to tuberculosis antigens (contained in TST or IGRA, or both) followed for at least 12 months. Following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) and meta-analyses of observational studies in epidemiology (MOOSE) guidelines, two reviewers independently extracted study data and assessed quality using a modified quality assessment of diagnostic accuracy studies (QUADAS-2) tool. Data were pooled using random effects generalised linear mixed models.
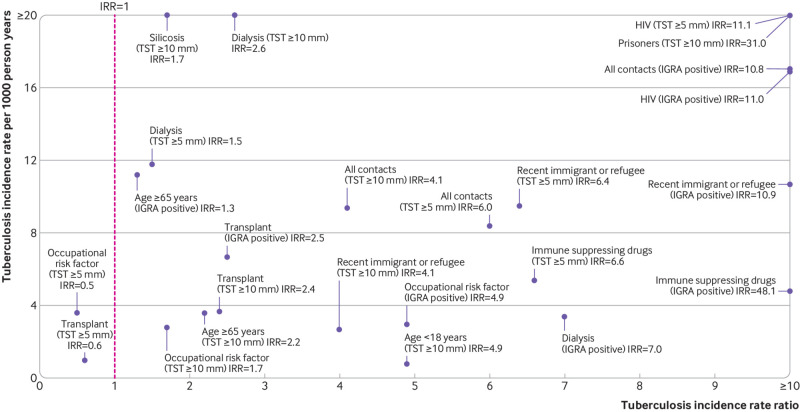
Main outcome measures: The primary outcome was tuberculosis incidence per 1000 person years among untreated participants who tested positive (TST or IGRA, or both) in different at risk subgroups. Secondary outcomes were the cumulative incidence of tuberculosis and incidence rate ratios among participants with a positive test result for latent tuberculosis infection compared with those with a negative test result in at risk subgroups.
Results: 122 of 5166 identified studies were included. In three general population studies, the incidence of tuberculosis among 33 811 participants with a TST induration of ≥10 mm was 0.3 (95% confidence interval 0.1 to 1.1) per 1000 person years. Among 116 197 positive test results for latent tuberculosis infection in 19 different at risk populations, incidence rates were consistently higher than those in the general population. Among all types of tuberculosis contacts, the incidence of tuberculosis was 17.0 (95% confidence interval 12.9 to 22.4) per 1000 person years for participants with a positive IGRA result and 8.4 (5.6 to 12.6) per 1000 person years for participants with a positive TST result of ≥5 mm. Among people living with HIV, the incidence of tuberculosis was 16.9 (10.5 to 27.3) for participants with a positive IGRA result and 27.1 (15.0 to 49.0) for participants with a positive TST result of ≥5 mm. Rates were also high for immigrants, people with silicosis or requiring dialysis, transplant recipients, and prisoners. Incidence rate ratios among test positive versus test negative participants were significantly greater than 1.0 in almost all risk groups, for all tests.
Conclusions: The incidence of tuberculosis is substantial in numerous at risk populations after a positive TST or IGRA result. The information from this review should help inform clinical decisions to test and treat for latent tuberculosis infection.
Study registration: PROSPERO CRD42019136608.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure and declare: JRC is supported by a postdoctoral fellowship from the Fonds de Recherche du Québec Santé (award #258907) and NW is supported through a Canadian Institutes of Health Research grant (FRD331745); no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Interferon-Gamma Release Assay Testing for Latent Tuberculosis Infection: A Health Technology Assessment.Ont Health Technol Assess Ser. 2024 Dec 12;24(11):1-183. eCollection 2024. Ont Health Technol Assess Ser. 2024. PMID: 39911267 Free PMC article.
-
The diagnostic performance of novel skin-based in-vivo tests for tuberculosis infection compared with purified protein derivative tuberculin skin tests and blood-based in vitro interferon-γ release assays: a systematic review and meta-analysis.Lancet Infect Dis. 2022 Feb;22(2):250-264. doi: 10.1016/S1473-3099(21)00261-9. Epub 2021 Oct 1. Lancet Infect Dis. 2022. PMID: 34606768
-
Interferon-γ release assays or tuberculin skin test for detection and management of latent tuberculosis infection: a systematic review and meta-analysis.Lancet Infect Dis. 2020 Dec;20(12):1457-1469. doi: 10.1016/S1473-3099(20)30276-0. Epub 2020 Jul 13. Lancet Infect Dis. 2020. PMID: 32673595
-
Interferon-γ release assay as a sensitive diagnostic tool of latent tuberculosis infection in patients with HIV: a cross-sectional study.BMC Infect Dis. 2018 Nov 19;18(1):585. doi: 10.1186/s12879-018-3508-8. BMC Infect Dis. 2018. PMID: 30453903 Free PMC article.
-
Contribution of a heparin-binding haemagglutinin interferon-gamma release assay to the detection of Mycobacterium tuberculosis infection in HIV-infected patients: comparison with the tuberculin skin test and the QuantiFERON-TB Gold In-tube.BMC Infect Dis. 2015 Feb 14;15:59. doi: 10.1186/s12879-015-0796-0. BMC Infect Dis. 2015. PMID: 25886172 Free PMC article.
Cited by
-
Latent tuberculosis infection in myasthenia gravis patients on immunosuppressive therapy: high incidence yet moderate reactivation rate.Ann Med. 2023;55(2):2282182. doi: 10.1080/07853890.2023.2282182. Epub 2023 Nov 14. Ann Med. 2023. PMID: 38375813 Free PMC article.
-
Burden of Chronic Obstructive Pulmonary Disease Attributable to Tuberculosis: A Microsimulation Study.Am J Epidemiol. 2023 Jun 2;192(6):908-915. doi: 10.1093/aje/kwad042. Am J Epidemiol. 2023. PMID: 36813297 Free PMC article.
-
Latent tuberculosis testing through the ages: the search for a sleeping killer.Am J Physiol Lung Cell Mol Physiol. 2022 Mar 1;322(3):L412-L419. doi: 10.1152/ajplung.00217.2021. Epub 2022 Feb 16. Am J Physiol Lung Cell Mol Physiol. 2022. PMID: 35170334 Free PMC article. Review.
-
Incidence and Risk Factors Associated with Latent Tuberculosis Infection and Pulmonary Tuberculosis among People Deprived of Liberty in Colombian Prisons.Am J Trop Med Hyg. 2021 Dec 6;106(1):66-74. doi: 10.4269/ajtmh.20-0307. Am J Trop Med Hyg. 2021. PMID: 34872056 Free PMC article.
-
The Growing Importance of Tuberculosis Preventive Therapy and How Research and Innovation Can Enhance Its Implementation on the Ground.Trop Med Infect Dis. 2020 Apr 16;5(2):61. doi: 10.3390/tropicalmed5020061. Trop Med Infect Dis. 2020. PMID: 32316300 Free PMC article.
References
-
- American Thoracic Society Targeted tuberculin testing and treatment of latent tuberculosis infection. MMWR Recomm Rep 2000;49(RR-6):1-51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources