

In Vivo Targeting of Clostridioides difficile Using Phage-Delivered CRISPR-Cas3 Antimicrobials
- PMID: 32156803
- PMCID: PMC7064742
- DOI: 10.1128/mBio.00019-20
In Vivo Targeting of Clostridioides difficile Using Phage-Delivered CRISPR-Cas3 Antimicrobials
Abstract
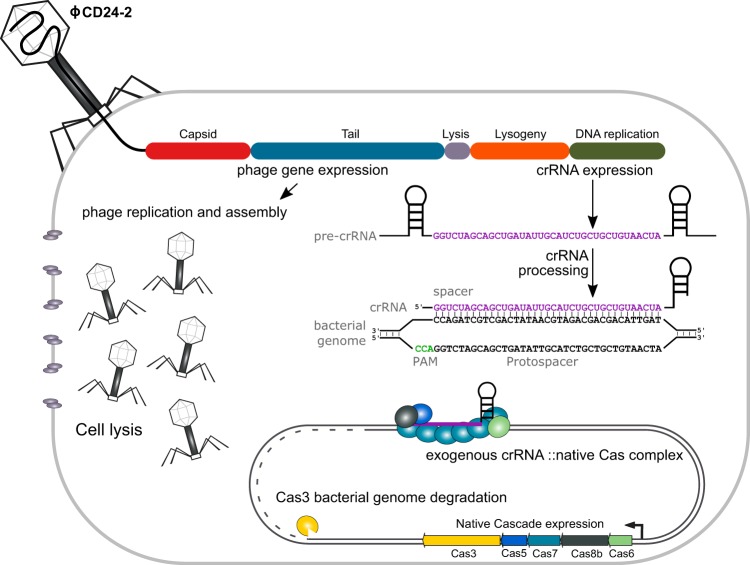
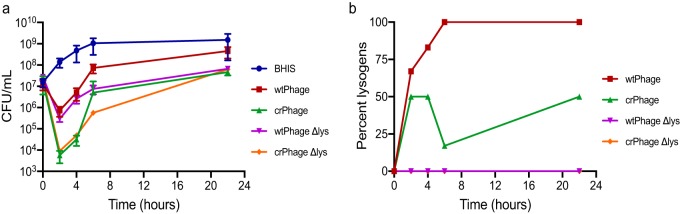
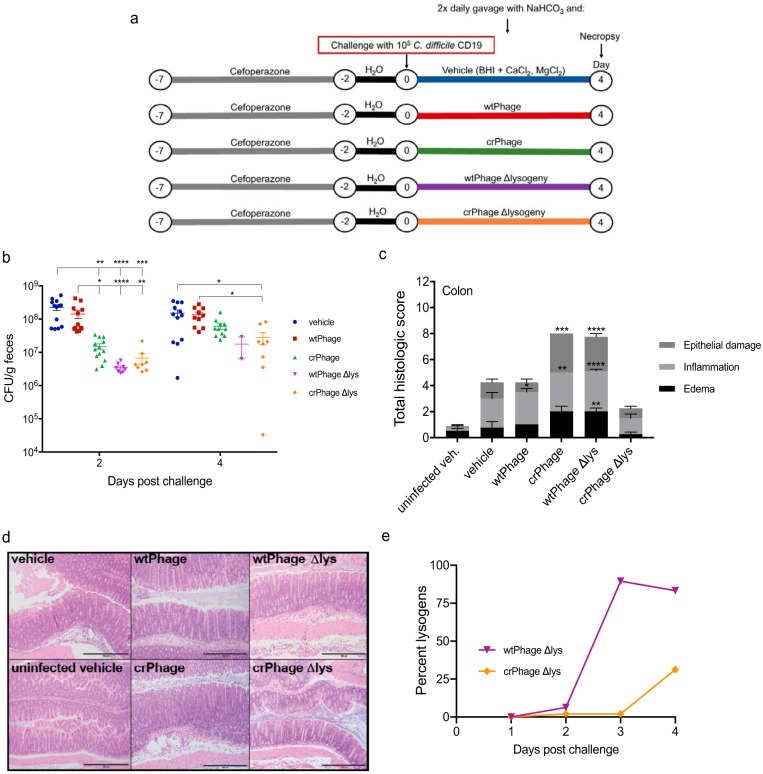
Clostridioides difficile is an important nosocomial pathogen that causes approximately 500,000 cases of C. difficile infection (CDI) and 29,000 deaths annually in the United States. Antibiotic use is a major risk factor for CDI because broad-spectrum antimicrobials disrupt the indigenous gut microbiota, decreasing colonization resistance against C. difficile Vancomycin is the standard of care for the treatment of CDI, likely contributing to the high recurrence rates due to the continued disruption of the gut microbiota. Thus, there is an urgent need for the development of novel therapeutics that can prevent and treat CDI and precisely target the pathogen without disrupting the gut microbiota. Here, we show that the endogenous type I-B CRISPR-Cas system in C. difficile can be repurposed as an antimicrobial agent by the expression of a self-targeting CRISPR that redirects endogenous CRISPR-Cas3 activity against the bacterial chromosome. We demonstrate that a recombinant bacteriophage expressing bacterial genome-targeting CRISPR RNAs is significantly more effective than its wild-type parent bacteriophage at killing C. difficile both in vitro and in a mouse model of CDI. We also report that conversion of the phage from temperate to obligately lytic is feasible and contributes to the therapeutic suitability of intrinsic C. difficile phages, despite the specific challenges encountered in the disease phenotypes of phage-treated animals. Our findings suggest that phage-delivered programmable CRISPR therapeutics have the potential to leverage the specificity and apparent safety of phage therapies and improve their potency and reliability for eradicating specific bacterial species within complex communities, offering a novel mechanism to treat pathogenic and/or multidrug-resistant organisms.IMPORTANCEClostridioides difficile is a bacterial pathogen responsible for significant morbidity and mortality across the globe. Current therapies based on broad-spectrum antibiotics have some clinical success, but approximately 30% of patients have relapses, presumably due to the continued perturbation to the gut microbiota. Here, we show that phages can be engineered with type I CRISPR-Cas systems and modified to reduce lysogeny and to enable the specific and efficient targeting and killing of C. difficilein vitro and in vivo. Additional genetic engineering to disrupt phage modulation of toxin expression by lysogeny or other mechanisms would be required to advance a CRISPR-enhanced phage antimicrobial for C. difficile toward clinical application. These findings provide evidence into how phage can be combined with CRISPR-based targeting to develop novel therapies and modulate microbiomes associated with health and disease.
Keywords: CRISPR; CRISPR-Cas; Cas3; Clostridioides difficile; lysogeny; phage.
Copyright © 2020 Selle et al.
Figures
References
-
- Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. 2015. Burden of Clostridium difficile infection in the United States. N Engl J Med 372:825–834. doi: 10.1056/NEJMoa1408913. - DOI - PMC - PubMed
-
- Magill SS, O'Leary E, Janelle SJ, Thompson DL, Dumyati G, Nadle J, Wilson LE, Kainer MA, Lynfield R, Greissman S, Ray SM, Beldavs Z, Gross C, Bamberg W, Sievers M, Concannon C, Buhr N, Warnke L, Maloney M, Ocampo V, Brooks J, Oyewumi T, Sharmin S, Richards K, Rainbow J, Samper M, Hancock EB, Leaptrot D, Scalise E, Badrun F, Phelps R, Edwards JR, Emerging Infections Program Hospital Prevalence Survey Team. 2018. Changes in prevalence of health care-associated infections in U.S. hospitals. N Engl J Med 379:1732–1744. doi: 10.1056/NEJMoa1801550. - DOI - PMC - PubMed
-
- McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, Dubberke ER, Garey KW, Gould CV, Kelly C, Loo V, Shaklee Sammons J, Sandora TJ, Wilcox MH. 2018. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 66:e1–e48. doi: 10.1093/cid/cix1085. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
