

Chemokine releasing particle implants for trapping circulating prostate cancer cells
- PMID: 32157115
- PMCID: PMC7064596
- DOI: 10.1038/s41598-020-60696-x
Chemokine releasing particle implants for trapping circulating prostate cancer cells
Abstract
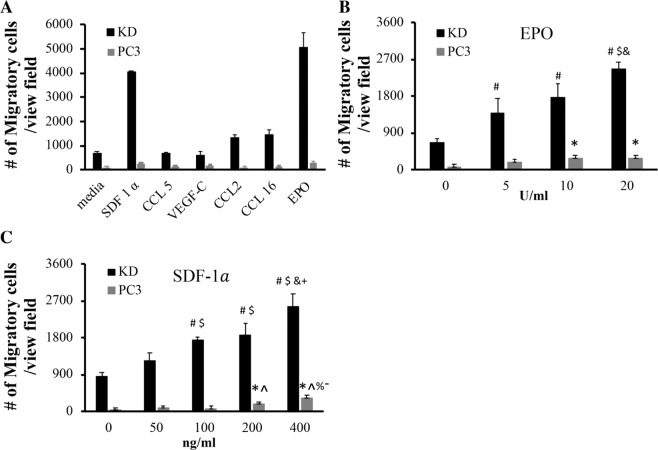
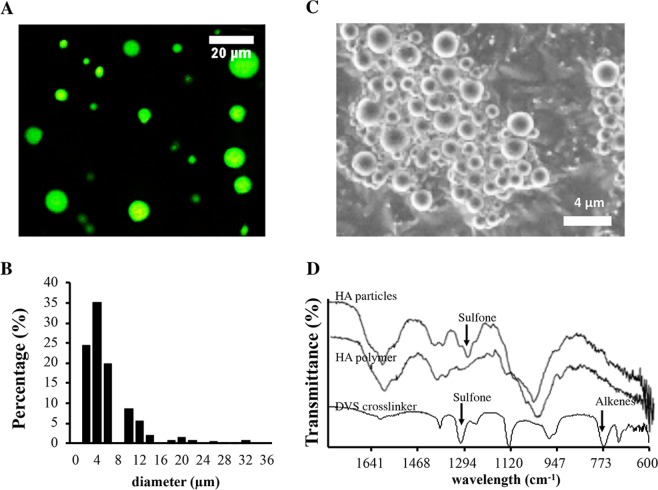
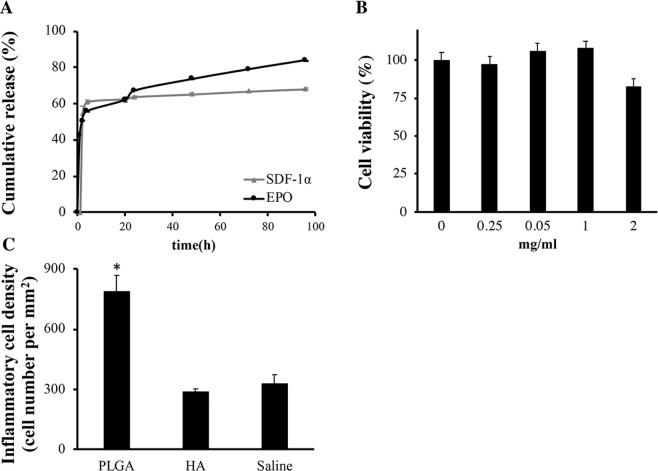
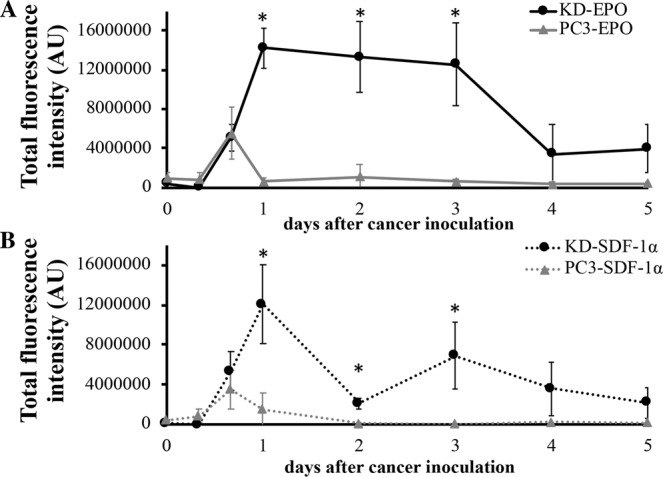
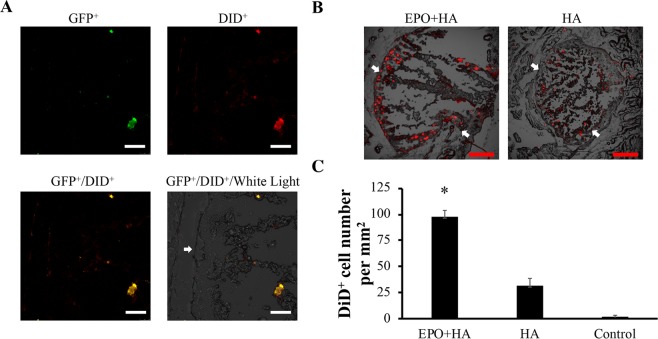
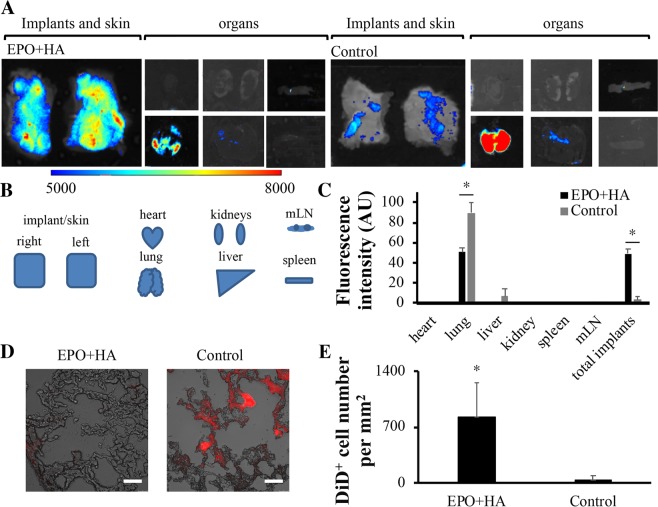
Prostate cancer (PCa) is the most prevalent cancer in U.S. men and many other countries. Although primary PCa can be controlled with surgery or radiation, treatment options of preventing metastatic PCa are still limited. To develop a new treatment of eradicating metastatic PCa, we have created an injectable cancer trap that can actively recruit cancer cells in bloodstream. The cancer trap is composed of hyaluronic acid microparticles that have good cell and tissue compatibility and can extend the release of chemokines to 4 days in vitro. We find that erythropoietin (EPO) and stromal derived factor-1α can attract PCa in vitro. Animal results show that EPO-releasing cancer trap attracted large number of circulating PCa and significantly reduced cancer spreading to other organs compared with controls. These results support that cancer trap may serve as a unique device to sequester circulating PCa cells and subsequently reduce distant metastasis.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
CXCR4 pharmacogical inhibition reduces bone and soft tissue metastatic burden by affecting tumor growth and tumorigenic potential in prostate cancer preclinical models.Prostate. 2015 Sep;75(12):1227-46. doi: 10.1002/pros.23007. Epub 2015 Jun 12. Prostate. 2015. PMID: 26073897
-
Suppression of prostate cancer cell rolling and adhesion to endothelium by 1α,25-dihydroxyvitamin D3.Am J Pathol. 2011 Feb;178(2):872-80. doi: 10.1016/j.ajpath.2010.10.036. Am J Pathol. 2011. PMID: 21281819 Free PMC article.
-
E-selectin ligand-1 controls circulating prostate cancer cell rolling/adhesion and metastasis.Oncotarget. 2014 Dec 15;5(23):12097-110. doi: 10.18632/oncotarget.2503. Oncotarget. 2014. PMID: 25301730 Free PMC article.
-
The origin of prostate metastases: emerging insights.Cancer Metastasis Rev. 2015 Dec;34(4):765-73. doi: 10.1007/s10555-015-9597-6. Cancer Metastasis Rev. 2015. PMID: 26363603 Review.
-
Disseminated tumor cells and dormancy in prostate cancer metastasis.Curr Opin Biotechnol. 2016 Aug;40:9-15. doi: 10.1016/j.copbio.2016.02.002. Epub 2016 Feb 20. Curr Opin Biotechnol. 2016. PMID: 26900985 Free PMC article. Review.
Cited by
-
CXCL12-loaded-hydrogel (CLG): A new device for metastatic circulating tumor cells (CTCs) capturing and characterization.Heliyon. 2024 Jul 31;10(15):e35524. doi: 10.1016/j.heliyon.2024.e35524. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39170328 Free PMC article.
-
Role of αVβ3 in Prostate Cancer: Metastasis Initiator and Important Therapeutic Target.Onco Targets Ther. 2020 Jul 28;13:7411-7422. doi: 10.2147/OTT.S258252. eCollection 2020. Onco Targets Ther. 2020. PMID: 32801764 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
